Session Information
Date: Monday, November 18, 2024
Title: SpA Including PsA – Diagnosis, Manifestations, & Outcomes Poster III
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Diagnostic delays are common in psoriatic arthritis (PsA). Screening surveys administered in clinic can identify psoriasis patients at elevated risk for PsA who should be prioritized for a rheumatologic diagnostic evaluation. However, screening surveys are infrequently used in practice because clinicians lack time to administer the screening. This study aims to 1) determine the effectiveness of a direct to patient (D2P) screening approach in which screening surveys and referral recommendations are mailed directly to psoriasis patients and 2) to understand the educational value of the screening materials.
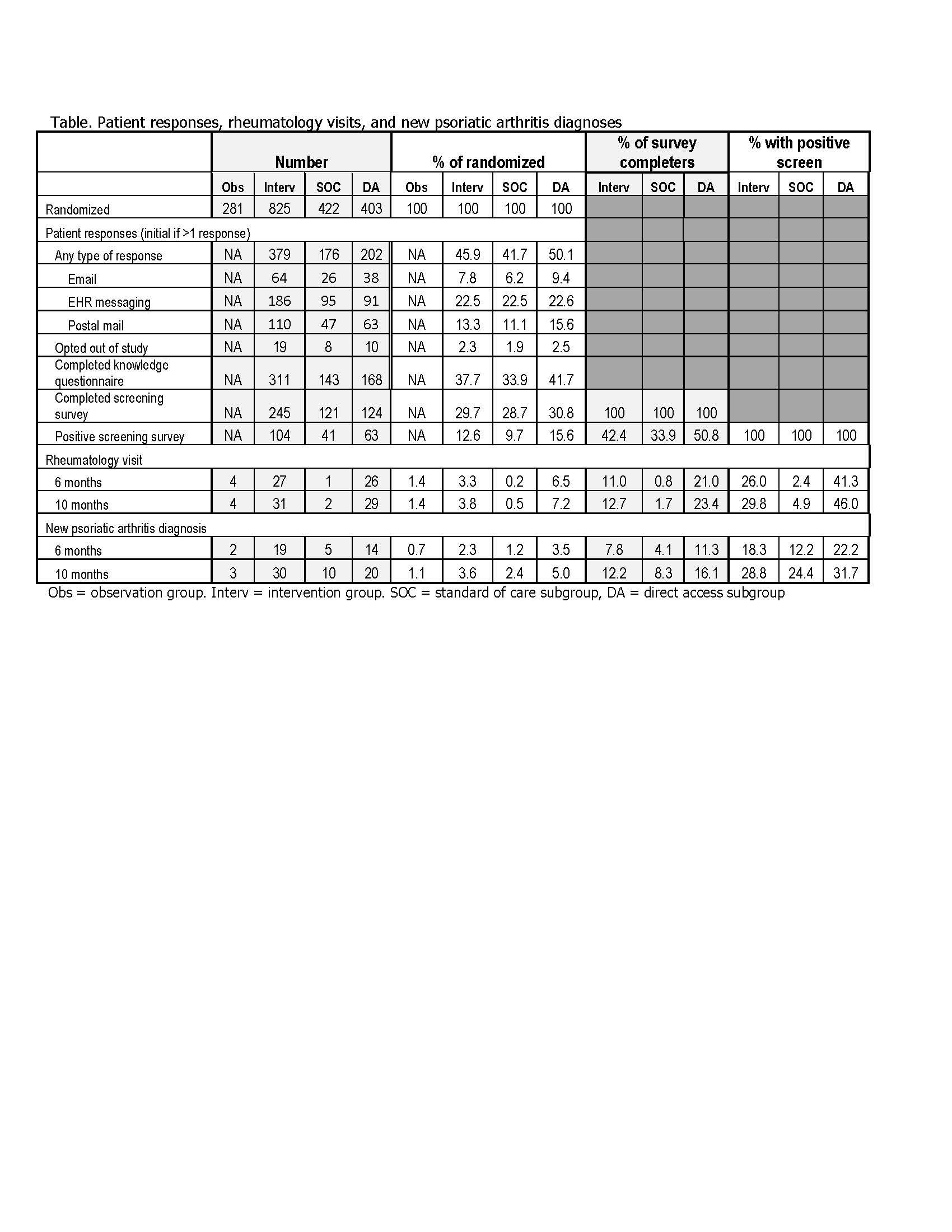
Methods: Patients from the University of Utah, who lived within 50 miles of the health center, with ≥2 diagnosis code for psoriasis between 11/15/2020-11/14/2022, without a PsA diagnosis code or rheumatology visit in their medical record, were randomized to an observation or intervention group. The intervention group consisted of the standard of care (SOC) and direct access (DA) subgroups. We mailed to the intervention group the Psoriasis Epidemiology Screening Tool (PEST) screening survey, educational materials, and a 2-item questionnaire assessing patients’ knowledge of PsA risk and the educational value of the screening materials by email, electronic health record (EHR) messaging, and postal mail. SOC patients who screened positive were advised to talk with their doctor about a referral to a rheumatologist and DA patients were advised to contact study staff for direct access to a rheumatology referral. We did not interact with the observation group. Outcomes from EHR data included the percentage of patients with a rheumatology visit or incident PsA diagnosis code at 6 months and 10 months after survey dissemination (index date).
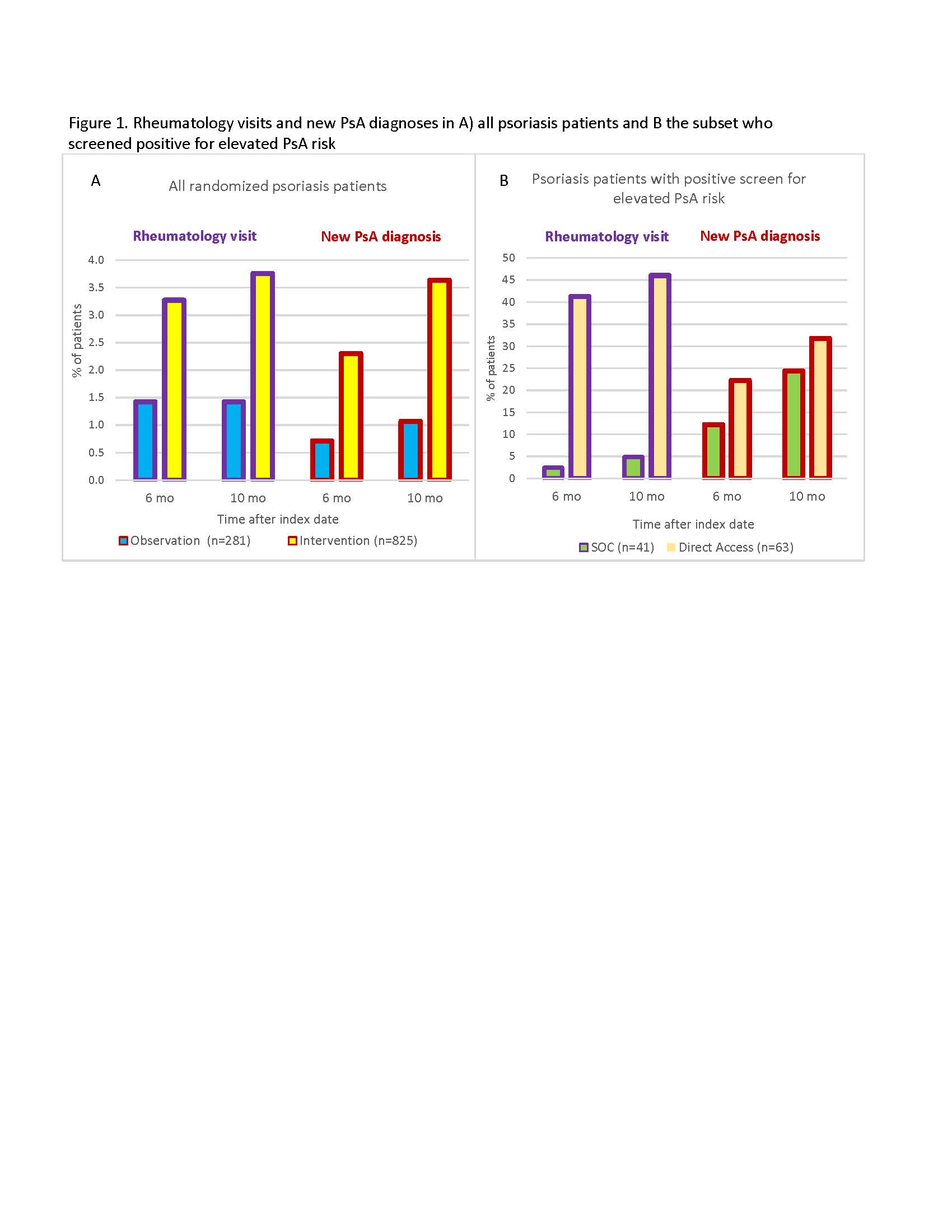
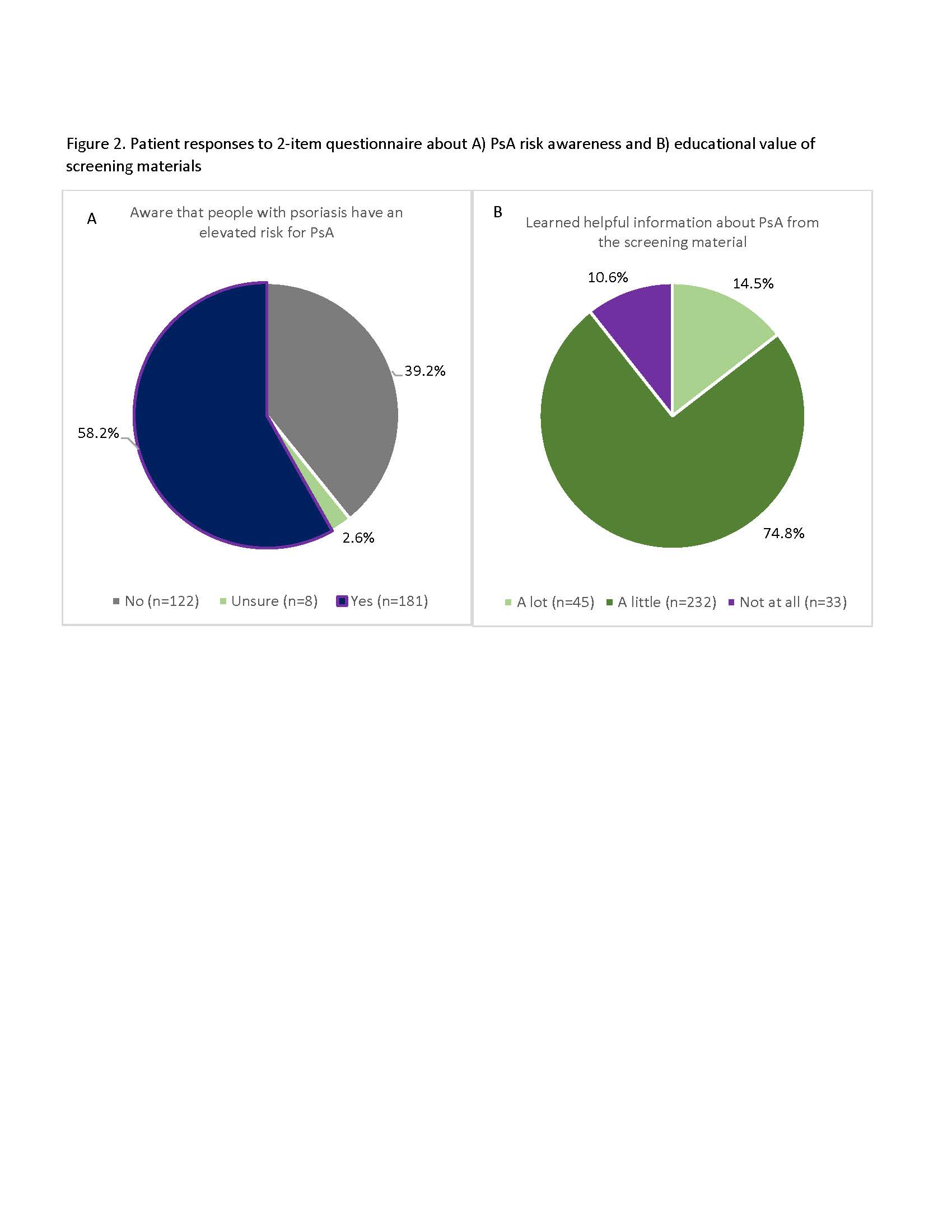
Results: The population included 53% females and 84% Caucasians, with a mean age was 54.9. The observation and intervention groups consisted of 281 and 825 patients, respectively. In the intervention group, 37.7% completed the knowledge questionnaire and 29.7% completed the screening survey (Table). Compared to the observation group, more patients in the intervention group had a rheumatology visit (3.3% vs. 1.4%) or a new PsA diagnosis (2.3% vs. 0.7%) 6 months after the index date (Figure 1). The mean times between index date and rheumatology visit were 3.4 months and 3.7 months in the DA and SOC subgroups, respectively. Among patients who screened positive by the PEST survey (n=104), a higher percentage in the DA than SOC subgroup had a rheumatology visit (41.3% vs. 2.4%) or a new PsA diagnosis (22.2% vs. 12.2%) at 6 months (Figure 2). Of the 311 patients who completed the knowledge questionnaire, 39.2% were unaware that people with psoriasis have an elevated risk for PsA and 89.4% learned a little or a lot about PsA from the screening materials.
Conclusion: The screening intervention increased rates of rheumatology visits and new PsA diagnoses by approximately 2-3 fold. Most of these visits and diagnoses occurred in the DA group, suggesting that ease of access to a rheumatology referral may substantially impact D2P screening strategies. There are unmet patient education needs about PsA risk, and nearly all patients indicated that the screening materials had educational value.
To cite this abstract in AMA style:
Walsh J, Pei S, Penmetsa G, Alexander S, Ly N, Molano-Romero R, Conlon A, Bakewell C, Reddy S, Scher J, Ogdie A. Direct to Patient Screening for Psoriatic Arthritis in Patients with Psoriasis: Diagnosis Rates, Referral Pathways, and Educational Value of Screening [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/direct-to-patient-screening-for-psoriatic-arthritis-in-patients-with-psoriasis-diagnosis-rates-referral-pathways-and-educational-value-of-screening/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/direct-to-patient-screening-for-psoriatic-arthritis-in-patients-with-psoriasis-diagnosis-rates-referral-pathways-and-educational-value-of-screening/