Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose:
Knee osteoarthritis (KOA) is one of the most common forms of arthritis and the most common cause of disability among the elderly. Knee pain is the presenting symptom of KOA, and symptomatic knee KOA is defined as “frequent knee pain” (pain on most days of at least one month in the past 12 months) and radiographic KOA. There is little data, however, on changes in knee pain over time. The purpose of this study was to identify whether there were different patterns of knee pain trajectories over four years of follow-up using data from the Osteoarthritis Initiative (OAI).
Methods:
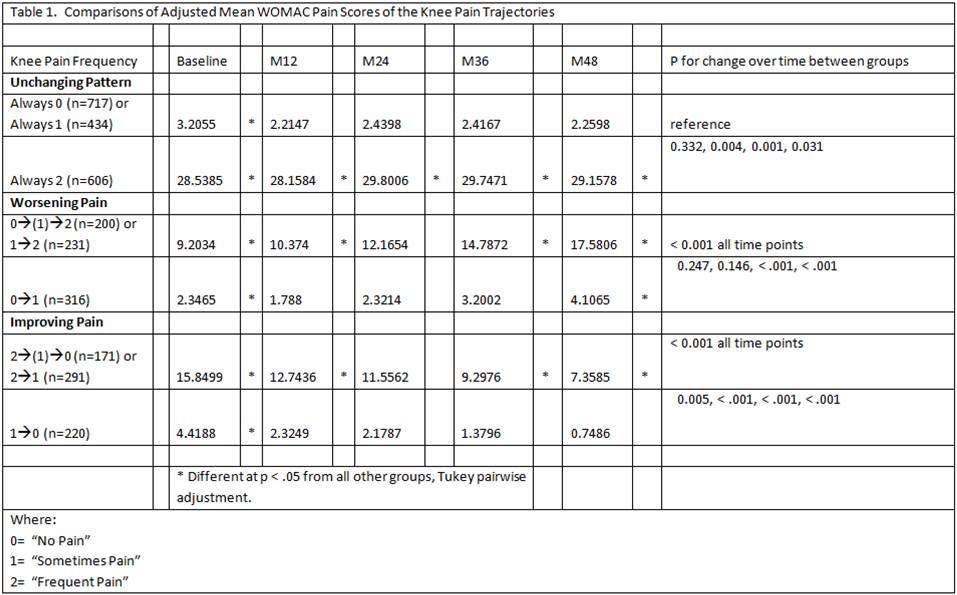
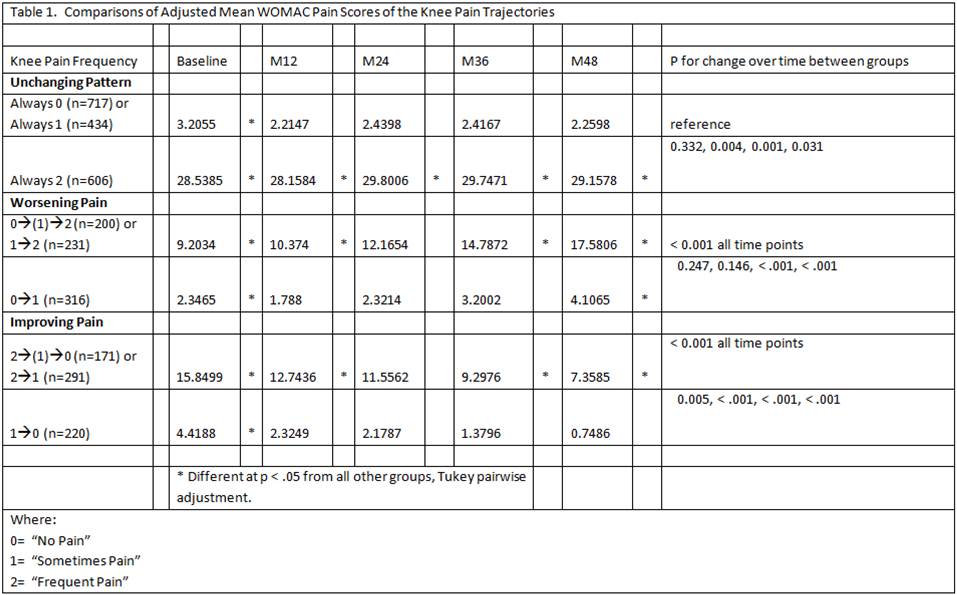
We studied 7,543 knees from OAI from baseline to 48 months (OAI public use data sets 2.1 and 2.2). Knee pain trajectories were based on the following knee pain reports at each visit: “No Pain” (no pain or aching in the past 12 months)=0, “Some Pain” (pain but not frequent pain)=1, or “Frequent Pain” (as above)=2. Unchanging subgroups had knees with same pain report at each visit: Group 1a, always 0; Group 1b, always 1; and Group 1c, always 2. Worsening subgroups had knees with consistent progression to worse pain: Group 2a for knees going 0–>(1)–>2; Group 2b 1–>2; and Group 2c 0–>1. Improving subgroups had knees with consistent progression to less pain: Group 3a for knees going from 2–>(1)–>0; Group 3b 2–>1; and Group 3c 1–>0. Fluctuating knee pain patterns (i.e., alternating between 0, 1 or 2 from visit to visit) were excluded from this analysis. To reduce the chances that a fluctuating knee was misclassified, for the worsening and improving subgroups, knees had to have two time points at the initial level of lower/higher pain or two time points at the final lower/higher level, respectively. Knee-specific WOMAC pain scores across the five visits were compared within each knee pain group using GEE (STATA 11.2) with each model adjusted for age, sex, race, educational level, depression, hand OA, and BMI. Subgroups within a group that were not distinct from each were combined. Comparison of differences between the larger subgroups was then performed.
Results:
Group 1a and Group 1b, Group 2a and Group 2b, Group 3a and Group 3b were no different from each other (p-values > 0.1). Each of these pairs was then collapsed into three respective subgroups. The results between remaining subgroups are summarized in Table 1 below. There were significant differences in the adjusted mean WOMAC pain scores at each OAI visit between the referent group (i.e., unchanging no/some pain) and the unchanging frequent pain subgroup, the worsening pain subgroups and the improving pain subgroups.
Conclusion:
We have been able to define distinct knee pain trajectories of unchanging, worsening and improving knee pain. Further work is underway to better characterize these groups. Better understanding of these knee pain trajectories may help to identify subgroups to target for specific interventions.
Disclosure:
J. Devich Jr.,
None;
M. J. Hannon,
None;
Z. Wang,
None;
R. M. Boudreau,
None;
C. K. Kwoh,
AstraZeneca,
2,
Beverage Institute,
2.
« Back to 2012 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/different-of-patterns-knee-pain-trajectories-longitudinal-data-from-the-osteoarthritis-initiative-oai/