Session Information
Date: Monday, November 18, 2024
Title: Vasculitis – Non-ANCA-Associated & Related Disorders Poster III
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Kawasaki disease (KD) is the leading cause of acquired heart disease in developed countries due to the development of coronary artery aneurysms (CAAs). Intravenous immunoglobulin (IVIG) is the primary initial treatment for KD, however treatment options for refractory KD (RKD), or KD requiring further treatment after the initial IVIG infusion, are not well defined. Predicting patients who will require immunomodulatory treatment in addition to IVIG is also challenging. We describe patients diagnosed with RKD at a large tertiary center to identify high risk features and effects of various treatment.
Methods: With IRB approval, we performed a retrospective chart review of patients diagnosed with RKD at our institution from 2017-2019. Demographics, clinical features, diagnostic findings, treatment, and outcomes were collected.
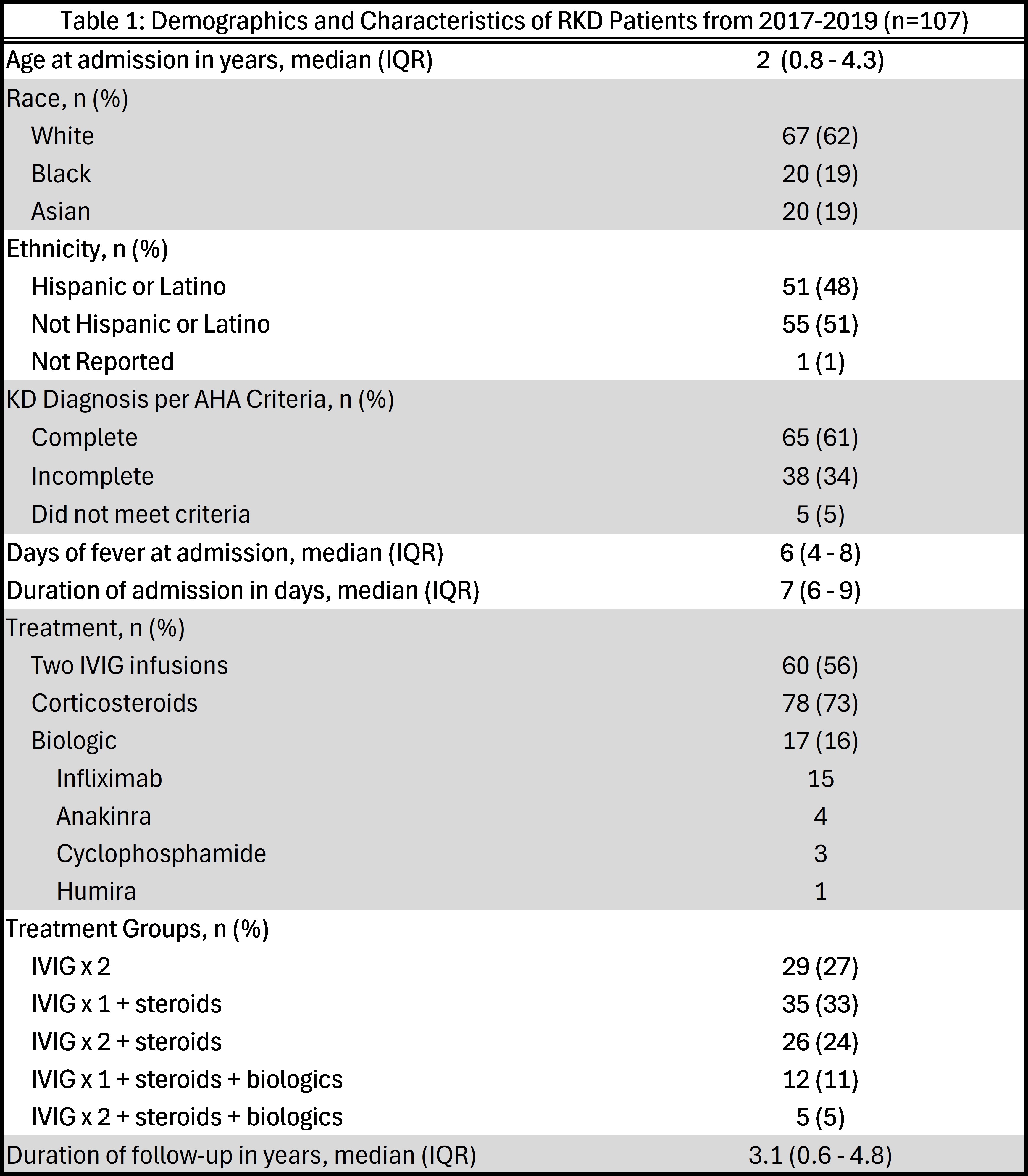
Results: Out of 312 patients diagnosed with KD, 107 (34%) had RKD with a racial/ethnic background of 62% White (48% Hispanic), 19% Black, and 19% Asian. The RKD patients had a median age of 2 years (IQR 0.8-4.3). As per American Heart Association (AHA) criteria, most RKD patients (61%) had complete KD, 34% had incomplete KD, and 5% did not meet criteria. CAAs were present in 68% of RKD patients with 49 patients developing small, 13 medium, and 11 giant aneurysms. Out of 107 patients, 56% received two IVIG infusions, 73% received corticosteroids, and 16% received biologic therapy. Two infusions of IVIG was the entire RKD treatment in 29 patients; the rest received a combination of IVIG with steroids and/or biologics.
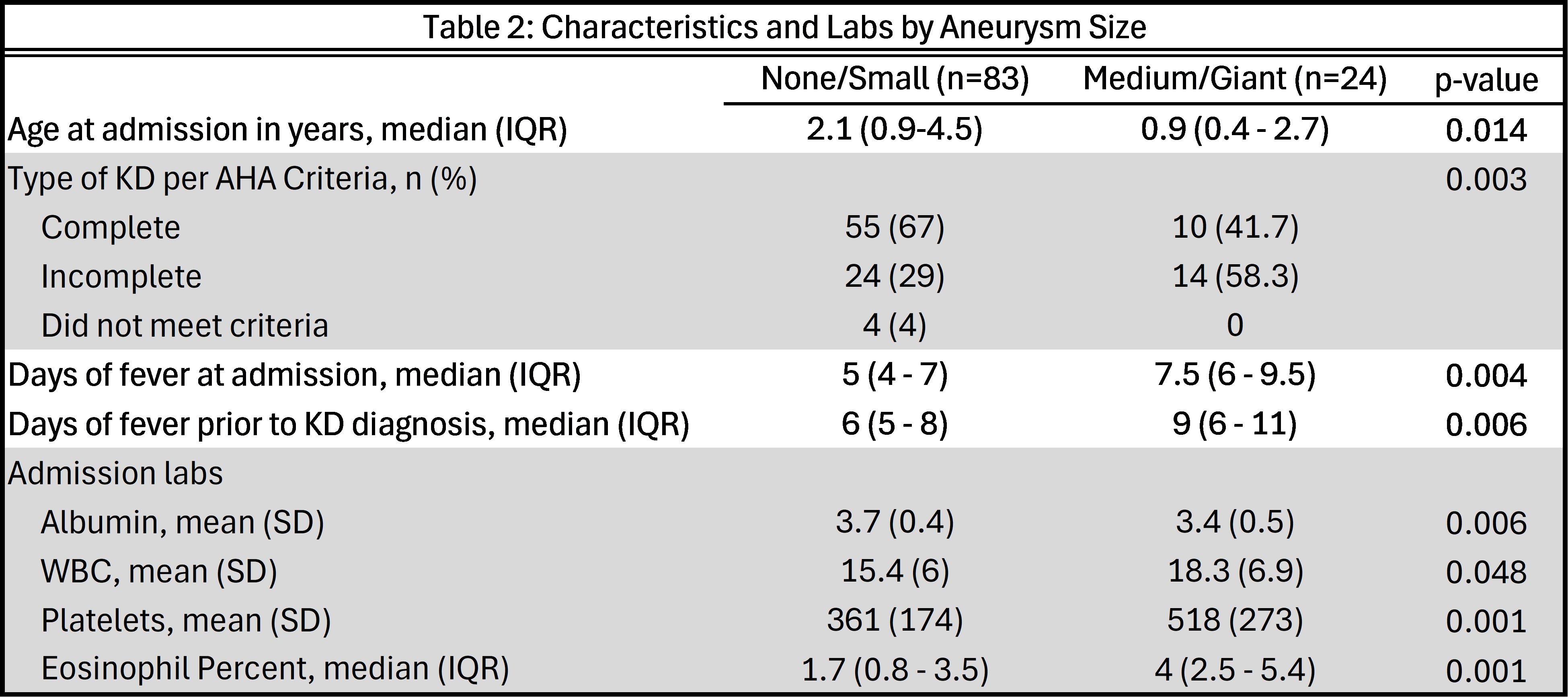
Patients with medium-to-giant CAAs were younger and had longer duration of fever prior to admission and before their KD diagnosis compared to patients with none or small CAAs (p < 0.05). Most patients with giant CAAs were Hispanic (91%, p = 0.03). A lower albumin and higher WBC, platelet, and eosinophil percentage at admission were noted in patients with medium-to-giant CAAs compared to patients with none or small CAAs (p < 0.05). CAAs did not correlate with CRP, d-dimer, or the Kobayashi score.
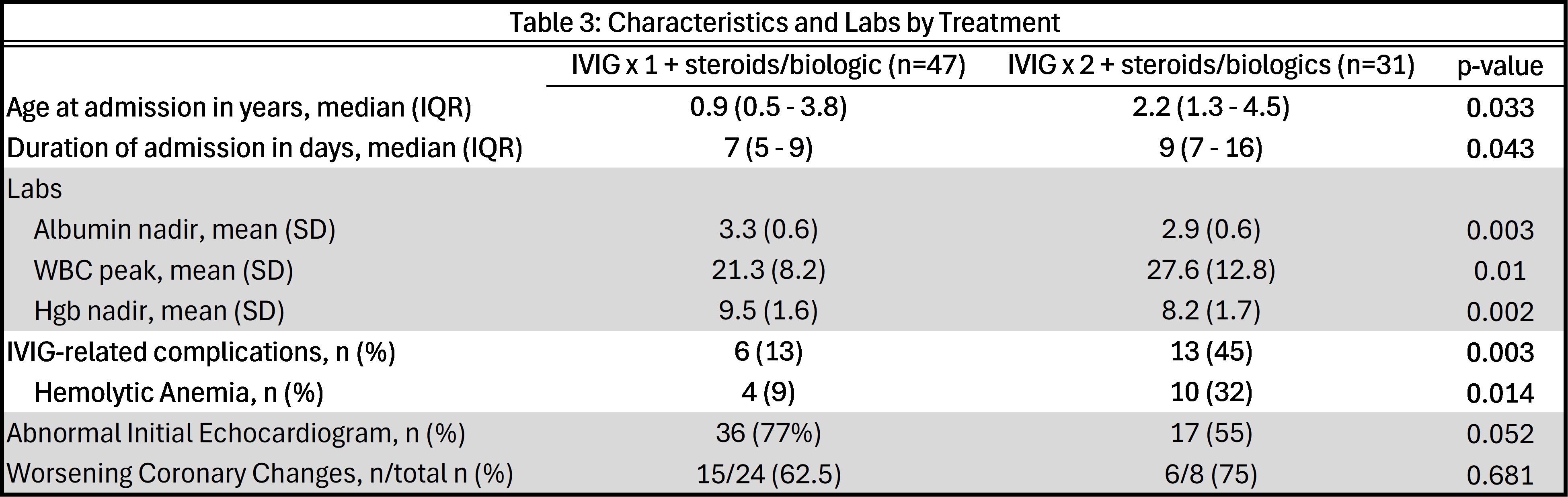
Two IVIG infusions with steroids and/or biologics was associated with longer hospital admissions, lower albumin and hemoglobin nadirs, higher WBC peak, and more IVIG-related adverse effects compared to one IVIG infusion with steroids and/or biologic (p < 0.05). However, rates of interventions required for IVIG-related adverse effects, such as transfusion for symptomatic anemia, were similar in both groups. There were no differences in worsening coronary changes between the groups.
Conclusion: This cohort of RKD patients represents a diverse, multiracial, and multiethnic population that has not been well-described in existing literature on RKD. Medium-to-giant aneurysms are associated with longer fever duration, lower albumin, and higher WBC, platelets, and eosinophil percent on admission. Giant aneurysms were almost exclusively seen in Hispanic patients. For patients who required steroid or biologic treatment for RKD, receiving two infusions of IVIG compared to one was associated with longer hospital admissions, more laboratory abnormalities, and more IVIG-related adverse effects. Therefore, our cohort suggests that use of a second IVIG infusion in patients with RKD should be reassessed.
To cite this abstract in AMA style:
Nguyen J, Guffey D, Ramirez A, Lai J, Vogel T, Sexson Tejtel S, Yildirim-Toruner C, DeGuzman M. Description of Patients with Refractory Kawasaki Disease at a Large Tertiary Center [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/description-of-patients-with-refractory-kawasaki-disease-at-a-large-tertiary-center/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/description-of-patients-with-refractory-kawasaki-disease-at-a-large-tertiary-center/