Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: 50-80% of children with childhood-onset systemic lupus erythematosus (cSLE) develop lupus nephritis (LN). Children from historically marginalized communities are disproportionately affected by cSLE and LN compared to their White counterparts, with higher prevalence and more severe LN outcomes. Adherence to these LN guidelines is not consistent. This study aims to investigate differences in adherence to guideline-recommended quality indicators among pediatric patients with LN based on factors such as race/ethnicity, age, comorbidity burden, and healthcare access.
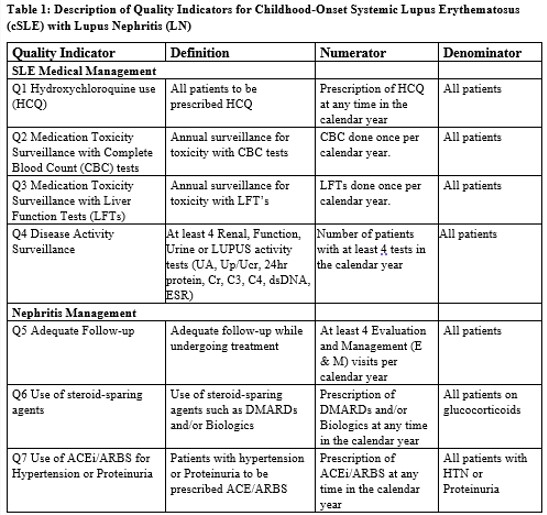
Methods: Using Medicaid via Marketscan data from 2011-2019, we identified individuals with LN between the ages of 5 and 21. Patients are required to ≥ 3 or more SLE ICD-9 or ICD-10 codes in outpatient visit claims or hospital discharge diagnosis codes at least 30 days apart and have ≥ 3 ICD-9/ICD-10 for nephritis and a procedure code for renal biopsy. Adherence to 7 LN quality indicators, were evaluated (Table 1). Multivariable analysis was performed to understand the association of race and ethnicity, comorbidities, age, and healthcare access with adherence to quality indicators.
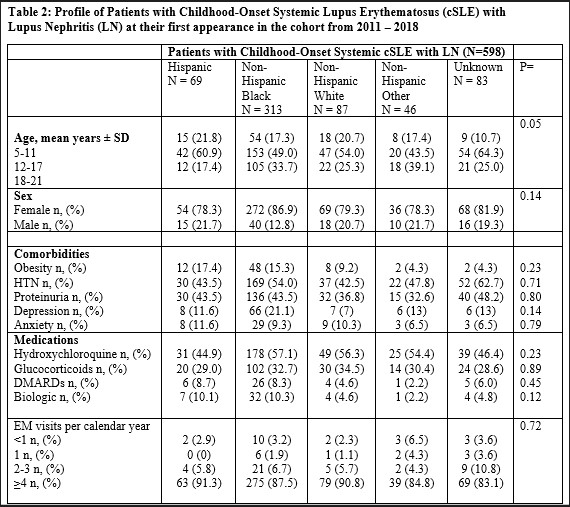
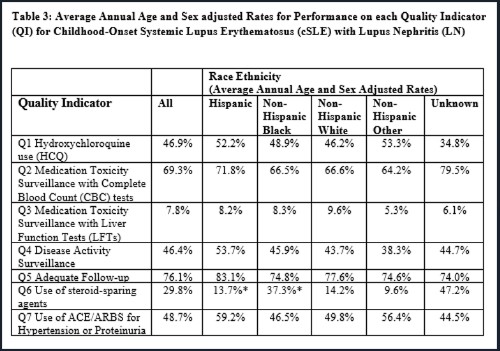
Results: We identified 598 children with prevalent childhood-onset LN;11.5% were Hispanic 52.3% Black, 14.5% White, 7.7% Unknown, 13.9% Other. (Table 2). Adherence to quality indicators was low (HCQ use: 46%, medication toxicity CBC: 69.3% LFT: 7.8%, disease activity monitoring: 46.4%, adequate follow-up: 76.1%, use of steroid-sparing agent: 29.8%, use of ACEi or ARB: 48.7%. No significant differences were noted by race/ethnicity. In the multivariable analysis, Black children and Other were associated with higher performance of HCQ use; RR 1.40, 95% CI (1.01-1.95) and RR 1.71, 95% CI (1.16-2.52), respectively. No other associations between race and ethnicity were noted. Older age (18-22 years old) was associated with lower performance of many quality indicators, which include HCQ use (RR 0.64, 95% CI [0.50-0.80]), disease activity surveillance labs (RR 0.66, 95% CI [ 0.56-0.78)] and ACEi/ARB use for HTN and proteinuria (RR 0.56, 95% CI [ 0.43-0.73]). Similarly, children with fewer visits in a year (1-4 visits) were associated with lower performance for HCQ use (RR 0.74, 95% CI 0.62-0.88), LFTs toxicity labs (RR 0.40, 95% CI 0.21-0.75), disease activity labs (RR 0.55, 95% CI 0.44-0.70), ACEi/ARB use (RR 0.63, 95% CI 0.52-0.76) (Table 3).
Conclusion: Our study suggests that children with prevalent LN and Medicaid coverage have poor adherence to LN quality indicators. There were no significant differences by race/ethnicity, but young adults had even lower adherence compared with younger children. Providers must include transition plans for young adults to ensure continuous quality care.
To cite this abstract in AMA style:
Akinsete A, Rajan M, Soroka O, Onel K, Safford M, Navarro Millan I. Delivery of Guideline Concordant Care in Childhood-Onset Lupus Nephritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/delivery-of-guideline-concordant-care-in-childhood-onset-lupus-nephritis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/delivery-of-guideline-concordant-care-in-childhood-onset-lupus-nephritis/