Session Information
Session Type: Abstract Session
Session Time: 2:15PM-2:30PM
Background/Purpose: Determining optimal cut-offs for active and structural imaging lesions of juvenile spondyloarthritis (JSpA) with axial disease is important for diagnosis, therapeutic management, and classification. We aimed to determine quantitative sacroiliac joint (SIJ) imaging lesion thresholds to 1. define a positive MRI for inflammatory and structural lesions typical of axial JSpA and 2. evaluate the lesions associated with assessment of axial disease by a panel of SpA experts.
Methods: Subjects were a retrospective cohort of children who had an MRI as part of their evaluation for suspected axial disease. MRI scans were reviewed by 6 central raters blinded to clinical details. Raters provided a yes/no response and confidence levels to the following parameters: 1) Are there typical active inflammatory lesions compatible with axial SpA present in the SIJs or at entheseal sites outside the SIJ? 2) Are typical chronic inflammatory lesions present in or around the SIJs? Raters assessed lesions in SIJ quadrants or halves on consecutive semi-coronal slices on a web-based interface for: a) bone marrow edema (BME), b) inflammation in erosion cavity, c) erosion, d) sclerosis, e) fat lesion, f) backfill, and g) ankylosis. Optimal sensitivity and specificity of MRI score cut-offs for each lesion were calculated using central imaging majority (≥4/6 raters) designation of high confidence (≥+3 on confidence scale from -5, “Definitely No”, to +5, “Definitely Yes”) in the presence of MRI active or structural lesions typical of axial SpA as the reference standard. All clinical and imaging data were assessed by 3 of 14 SpA expert panelists. JSpA experts assessed their confidence that the case was “JSpA with axial disease” with the anchors -3 (very unlikely) to +3 (very likely). Cases classified by majority (≥2/3) experts with high confidence (≥+2) were used as the reference standard. Test statistic properties of the quantitative lesion-based MRI thresholds were assessed against this reference standard.
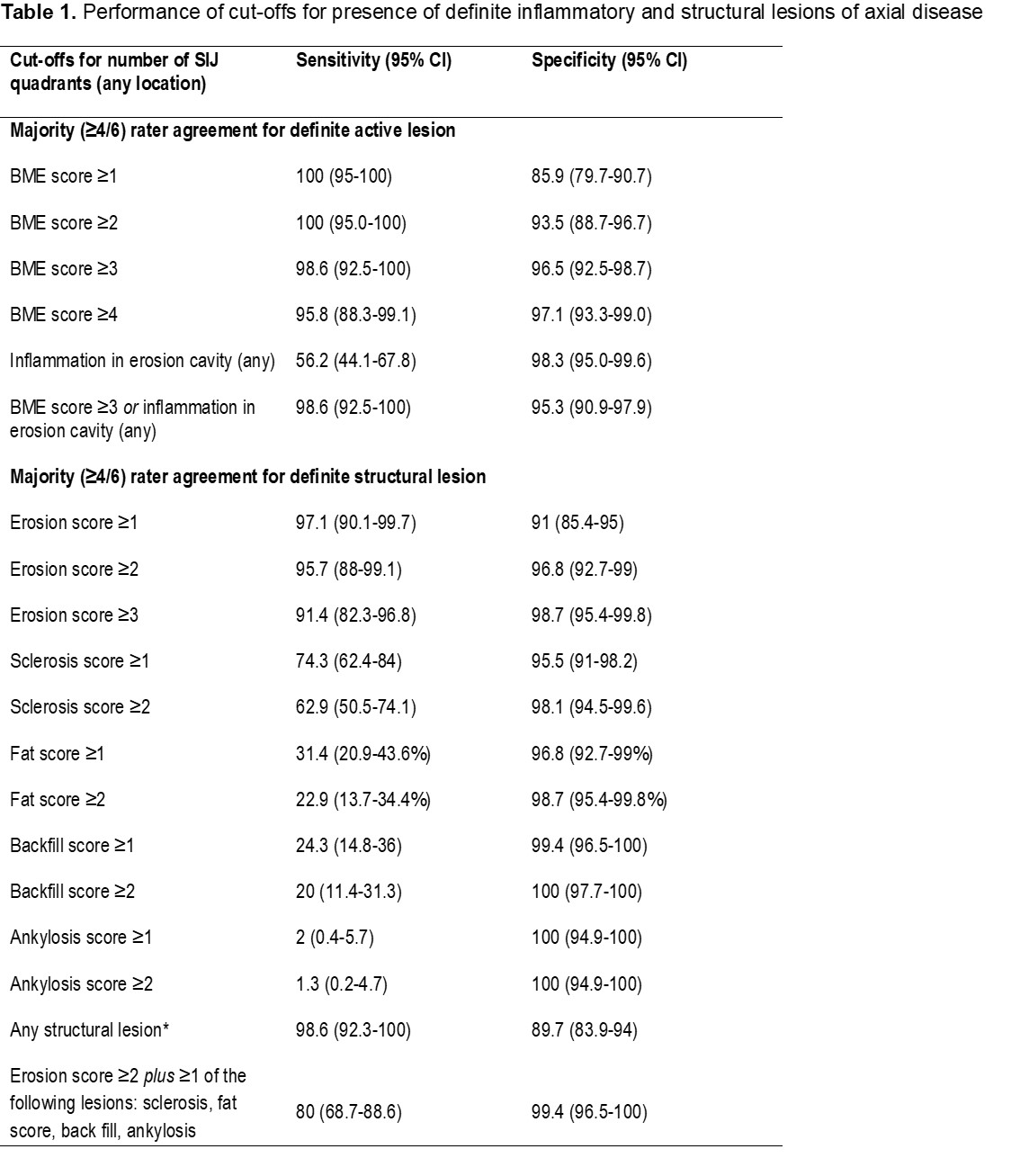
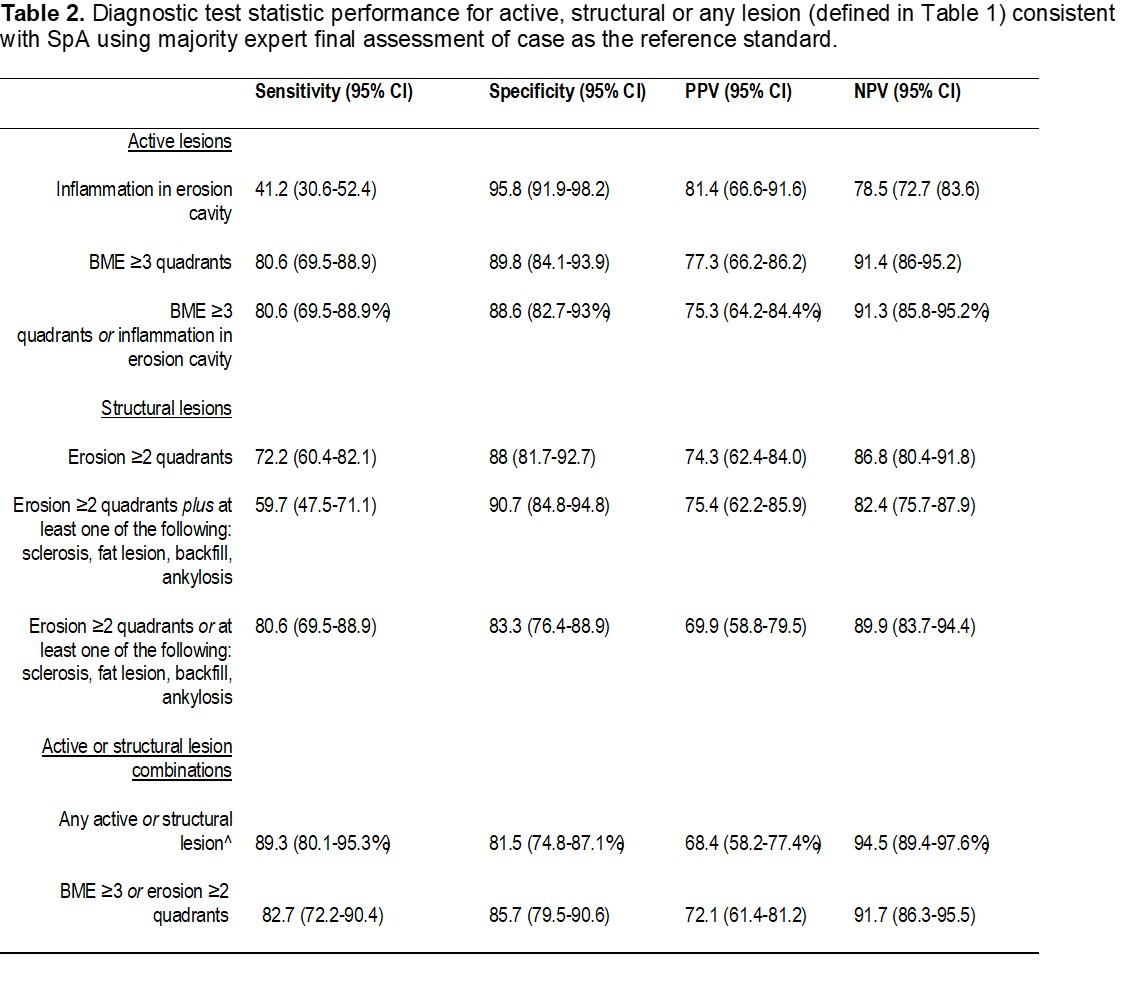
Results: Imaging from 243 subjects, 61% male, median age 14.9 had sequences available for detailed MRI scoring. The lesion-based cut-offs achieving specificity ≥95% with the highest sensitivity for a definite active inflammatory lesion were: BME in ≥3 quadrants or ≥1 inflammation in an erosion cavity (Table 1); combining the two types of lesions did not add incremental value. For definite structural lesion, the lesion cut-offs achieving ≥95% specificity with the highest sensitivity were the following: erosion in ≥2 quadrants, sclerosis in ≥1 quadrant, fat lesion in ≥1 quadrant, and backfill in ≥1 quadrant (Table 1); combinations of the lesions did not add incremental value. PPV and NPV of the quantitative threshold definitions for active, structural, or any lesions typical of axial SpA using the majority expert final assessment as the reference standard are shown in Table 2. The PPV and specificities were highest for BME ≥3 quadrants, erosion in ≥2 quadrants or a combination of the 2.
Conclusion: We propose cut-offs for definite active and structural lesions on MRI typical of axial disease in JSpA that have high PPV and specificity for clinical assessment. These cut-offs have applicability for diagnosis, therapeutic management, and classification.
To cite this abstract in AMA style:
Weiss P, Brandon T, Aggarwal A, Burgos-Vargas R, Colbert R, Horneff G, Joos R, Laxer R, Minden K, Ravelli A, Ruperto N, Smith J, Stoll M, Tse S, Van den Bosch F, Lambert R, Biko D, Chauvin N, Francavilla M, Jaremko J, Herregods N, Kasapcopur O, YILDIZ M, Hendry A, Maksymowych W. Data-driven MRI Definitions for Active and Structural Sacroiliac Joint Lesions in Juvenile Spondyloarthritis Typical of Axial Disease [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/data-driven-mri-definitions-for-active-and-structural-sacroiliac-joint-lesions-in-juvenile-spondyloarthritis-typical-of-axial-disease/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/data-driven-mri-definitions-for-active-and-structural-sacroiliac-joint-lesions-in-juvenile-spondyloarthritis-typical-of-axial-disease/