Session Information
Date: Monday, November 8, 2021
Session Type: Poster Session C
Session Time: 8:30AM-10:30AM
Background/Purpose: In a cohort of early rheumatoid arthritis (eRA) patients, we recently showed that early and aggressive treatment led to remission and limited erosive progression at 11 years. Anti-citrullinated protein antibody (ACPA), a high degree of inflammation (DAS28crp) and MRI bone marrow oedema predicted long term radiographic progression at 11 years (Scand J Rheumatol 2018, 48: 1-8). In this cohort, we investigated plasma levels of CXCL13, and its ability to predict radiographic joint destruction.
Methods: In a post-hoc study, a serial set of plasma samples was obtained from the investigator-initiated CIMESTRA study (n=117). CXCL13 was measured at baseline and after 1 year. Patients were characterized and monitored by C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), Disease Activity Score in 28 joint (DAS28), swollen joint count in 28 joints (SJC28), health assessment questionnaire (HAQ) and global visual analogue scales (VAS). IgM-rheumatoid factor (IgM-RF) and ACPA status was recorded at baseline. Cumulative dose of glucocorticoid injections was recorded. Radiographic status and progression were assessed by total Sharp Score (TSS) at baseline and 11 years. Data were analysed using Wilcoxon matched pairs-signed rank test (Median (25-75 percentile), multivariate regression analysis (coefficient +/- standard error), Spearman correlation (rho) and ROC curves, determining the threshold for radiographic damage as a score of 5, applicable for TSS and deltaTSS.
Results: In eRA patients, plasma levels of CXCL13 were increased (60 pg/ml (39-102) and decreased after one year of treatment (31 pg/ml (23-49) (p< 0.0001). By Spearman correlation analyses, baseline levels of CXCL13 were associated with CRP (0.50), ESR (0.49), ACPA (0.39), IgM-RF (0.38), VAS Global (0.27), HAQ (0.38), and DAS28CRP (0.27), all p< 0.05.
In a multivariate regression analysis, adjusting for smoking status, age, gender, ACPA status, CRP, number of glucocorticoid injections, SJC28 and ESR, baseline CXCL13 was associated with both TSS (0.11 +/- 0.04, p=0.004) and deltaTSS (0.07 +/- 0.03, p=0.042) after 11 years of treatment (Figure 1). The predictive value of baseline CXCL13 for TSS >5 at 11 years was illustrated in the ROC curve with an area under curve (AUC) of 0.72, p< 0.001 (Figure 2). AUC for DAS28CRP was: 0.58, p=0.2, for CRP: 0.64, p=0.02 and for ACPA: 0.59, p=0.34. Based on the ROC curve, selecting the highest possible sensitivity and specificity of both 70%, CXCL13 levels above 53 pg/ml predicted significant radiographic destruction after 11 years with a likelihood ratio of 2.3.
Numbers of glucocorticoid injections did not differ between patients with an 11-year TSS< 5 and TSS >5.
A similar analysis was done for baseline CXCL13 and deltaTSS at 11 years, also supporting a predictive value of baseline CXCL13 for radiographic progression (AUC=0.62, p=0.03).
Conclusion: Predicting long-term radiographic destruction in patients with newly diagnosed RA remains challenging. Here, we suggest plasma CXCL13 as a reliable marker of long-term disease severity in RA, especially predicting significant radiographic destruction after more than 10 years of treatment.
 Figure 1: Plot of baseline CXCL13 and TSS after 11 years of treatment.
Figure 1: Plot of baseline CXCL13 and TSS after 11 years of treatment.
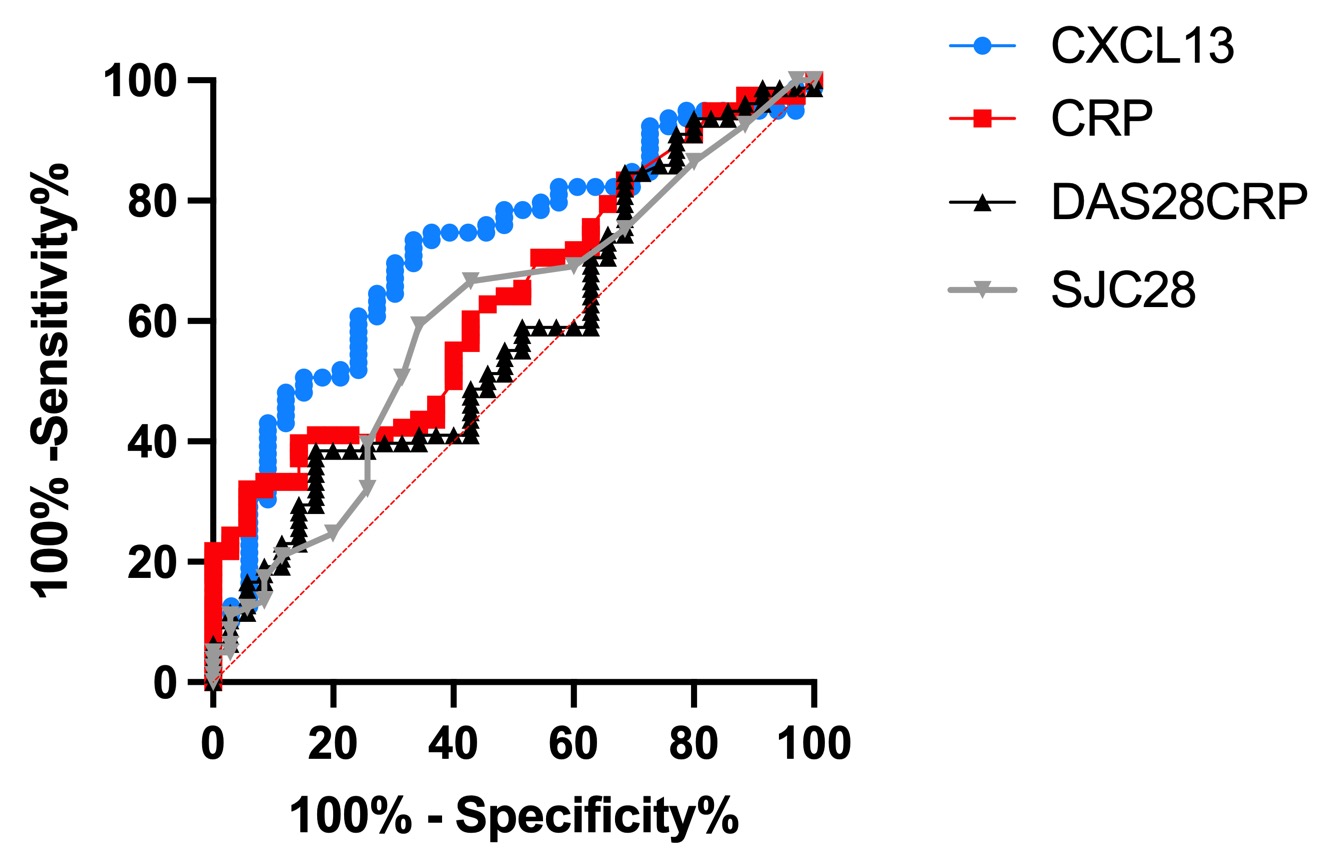 ROC curves of CXCL13, CRP, DAS28CRP and SJC28 predicting TSS above 5 after 11 years of treatment. A TSS score of 5 or above is considered as significant radiographic progression, as this accounts for one destroyed joint.
ROC curves of CXCL13, CRP, DAS28CRP and SJC28 predicting TSS above 5 after 11 years of treatment. A TSS score of 5 or above is considered as significant radiographic progression, as this accounts for one destroyed joint.
To cite this abstract in AMA style:
Greisen S, Hetland M, Ostergaard M, Horslev-Petersen K, Junker P, Stengaard-Petersen K, Hvid M, Deleuran B. CXCL13 Outranges DAS28CRP and CRP as Predictor of Long-term Radiographic Status in Early Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/cxcl13-outranges-das28crp-and-crp-as-predictor-of-long-term-radiographic-status-in-early-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/cxcl13-outranges-das28crp-and-crp-as-predictor-of-long-term-radiographic-status-in-early-rheumatoid-arthritis/