Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Ultrasound (US) allows for visualization of features of knee osteoarthritis (KOA) including osteophytes, meniscal extrusion, synovitis, and cartilage damage. The current analysis aimed to determine the association of features of KOA on US with patient reported symptoms and radiographic KOA (rKOA).
Methods: Data were from participants in the population-based Johnston County Health Study, who provided demographic information, symptomatic assessments, and imaging. Self-reported pain, aching or stiffness (PAS, 0-3, none to severe) was assessed on most days of any one month in the past 12 months. Posteroanterior semi-flexed radiographs were read for Kellgren Lawrence Grade (KLG) by an expert musculoskeletal radiologist (JBR). Standardized knee US images were obtained by a trained sonographer (SSG). Each set of images was read independently by 2 randomly selected expert readers (CJB, MJK, JL, JS); discrepancies were adjudicated by a 3rd independent reader. Knee outcome definitions included any knee PAS, at least moderate severity PAS, rKOA (KLG≥2), severe rKOA (KLG≥3), and symptomatic KOA (sxKOA, rKOA and any PAS).
We fitted logistic regression models to test the associations (adjusted odds ratios and 95% confidence intervals) between each US feature and KOA outcomes. Models were adjusted for age, sex, race, ethnicity, BMI, education, Charlson comorbidity index, and history of knee injury. Models were defined at the knee level so that generalized estimating equations were used to account for within-person correlation between knees. Effect modification between all covariables and US features was assessed using two-way interaction terms at a 0.05 alpha level and reported in stratified models.
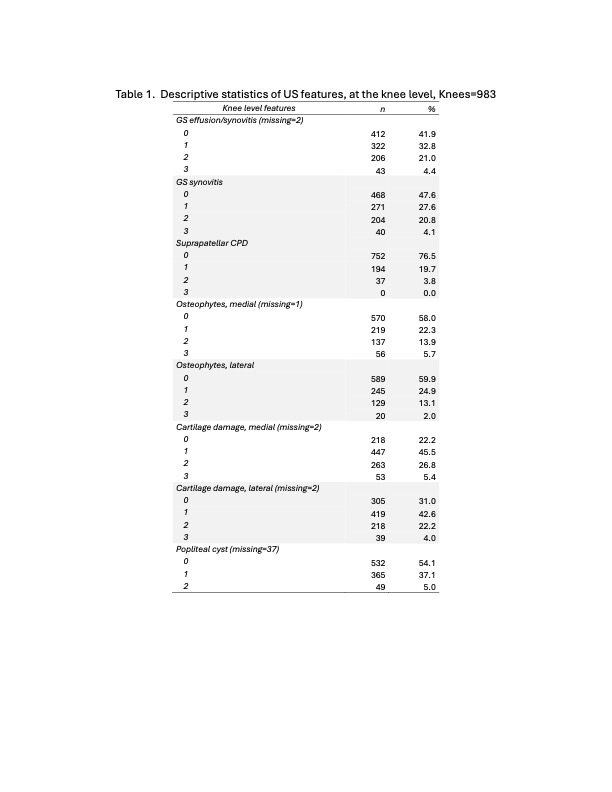
Results: A total of 499 individuals (35% men, 26% Black, 9% Hispanic, mean age 55 [range 35-70] years, mean BMI 33 kg/m2, and 51% with < college degree) with 983 knees, 313 (31%) of which had rKOA, were included. Cartilage damage and the presence of effusion/synovitis were the most frequent features of KOA on US (Table 1). Additionally, 37% had an effusion, 13-18% had meniscal extrusion/damage, and 11% had calcium crystal deposition.
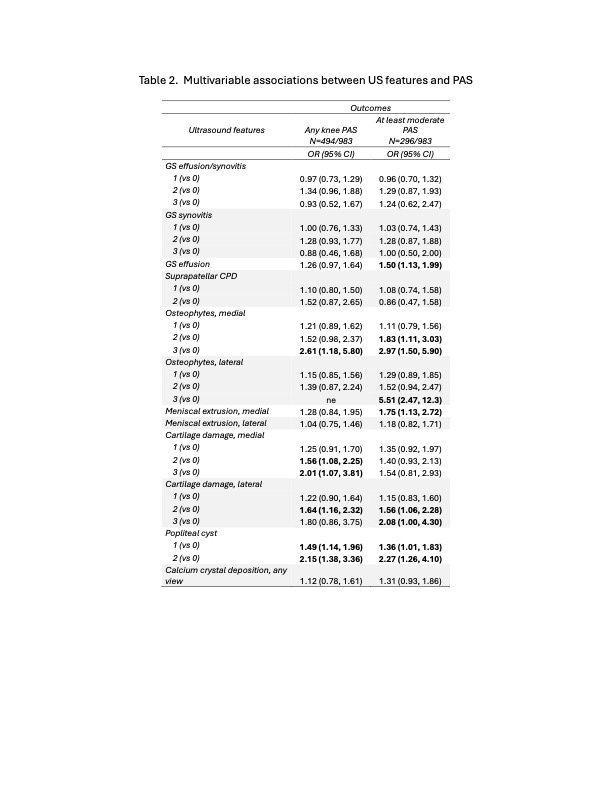
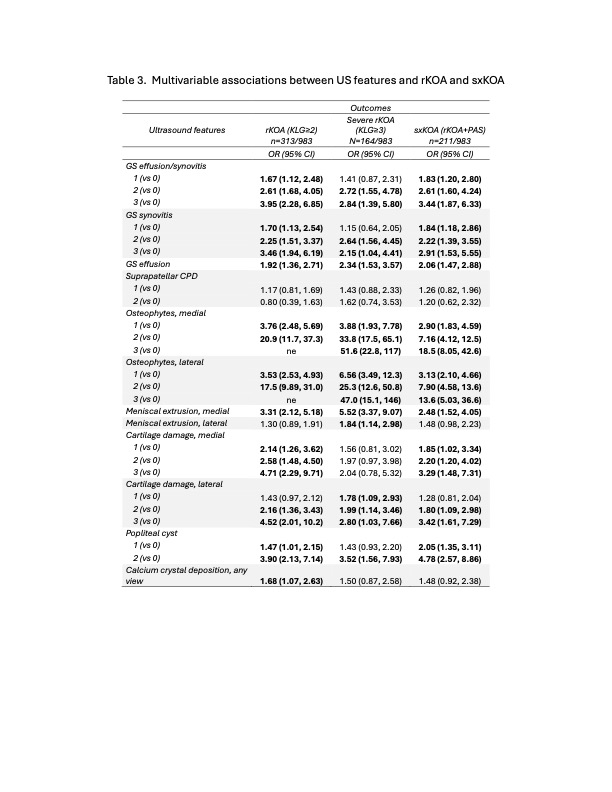
Large medial or lateral osteophytes or popliteal cysts were associated with any and at least moderate PAS (Table 2). Osteophytes, both medial and lateral, were strongly associated with rKOA, severe rKOA, and sxKOA. Smaller magnitude associations were observed with the presence of effusion/synovitis, cartilage damage, and popliteal cysts (Table 3).
Stratified models revealed a strong association between medial osteophytes and sxKOA for both men and women. Associations between lateral osteophytes and sxKOA appeared stronger in younger participants. Associations between effusion and rKOA, meniscal extrusion and PAS, and cartilage damage or popliteal cyst and severe rKOA, appeared stronger in men than in women (data not shown).
Conclusion: The presence of effusion/synovitis and osteophytes on US are commonly seen in KOA and strongly associated with higher KLG and patient reported symptoms. These US features can be assessed at bedside for the evaluation of KOA symptoms. It remains to be determined how these features may progress over time and their longitudinal impact on patient symptoms.
To cite this abstract in AMA style:
Yates K, Alvarez C, Sawani S, Arbeeva L, Schwartz T, Savage-Guin S, Renner J, Bakewell C, Kohler M, Lin J, Samuels J, Nelson A. Cross-sectional Associations Among Sonographic and Radiographic Features and Symptoms Scores in a Population-Based Cohort [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/cross-sectional-associations-among-sonographic-and-radiographic-features-and-symptoms-scores-in-a-population-based-cohort/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/cross-sectional-associations-among-sonographic-and-radiographic-features-and-symptoms-scores-in-a-population-based-cohort/