Session Information
Date: Monday, November 6, 2017
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: The regular assessment of disease activity is necessary to implement a treat-to-target management approach in RA. The Multi-Biomarker Disease Activity (MBDA) Score is a novel tool developed to facilitate RA disease activity assessment, but there have been conflicting reports on the ability of the MBDA score to assess RA disease activity. Therefore, we performed a systemic review of MBDA in RA and meta-analysis of the correlation between the MBDA and composite RA disease activity measures.
Methods: We conducted a systematic review and meta-analysis of published manuscripts on the MBDA in RA (registered with PROSPERO) by searching MEDLINE, EMBASE, Scopus, Google Scholar, and the Cochrane Library from their inception to March 7, 2017, adhering to the PRISMA guidelines. We included studies reporting correlations of MBDA with composite RA disease activity measures and completed a meta-analysis to calculate a pooled estimate. Studies only assessing MBDA performance in separate cohorts or time points were modeled as separate studies. We performed a random-effects meta-analysis of correlation coefficients using the DerSimonian-Laird model for measures assessed in ≥3 cohorts. In sensitivity analyses, we allowed each study to only contribute one cohort and transformed correlation coefficients to Fisher’s Z scores prior to meta-analysis. Heterogeneity was assessed using the Cochran Q test.
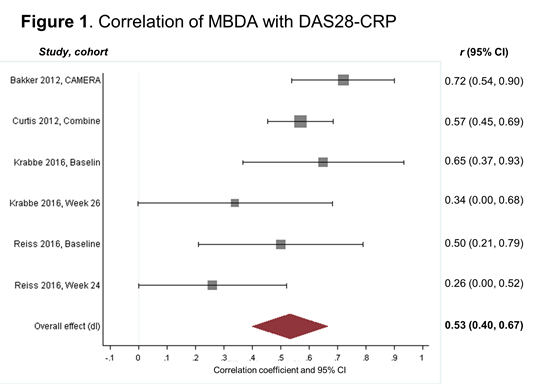
Results: The systematic review identified 18 reports examining the MBDA in RA, with 6 of these (n=9 cohorts) reporting correlations with composite RA disease activity measures. Results from meta-analysis demonstrated a moderate to strong correlation of the MBDA with DAS28-CRP (r=0.53, 95% CI 0.40-0.67, Figure 1). Heterogeneity was marginally significant by Cochrane Q (p = 0.07). Results were similar following conversion of correlation coefficients to Fisher’s Z scores (r=0.54, 95% CI 0.40-0.66) and using only one cohort (baseline) per study (r=0.61, 95% CI 0.52-0.70). The MBDA demonstrated similar correlations with the Simple Disease Activity Index (SDAI) and a slightly less robust correlation with the Clinical Disease Activity Index (CDAI) with significant heterogeneity across relevant studies (Table 1). There was a moderate to strong correlation between Δ-MBDA with Δ-DAS28-CRP (Table 1).
Conclusion: The MBDA demonstrates moderate to strong correlations with DAS28-CRP and SDAI, but less robust correlations with CDAI. Since CRP is a common component of MBDA, DAS28-CRP, and SDAI, additional study is needed to assess whether MBDA correlates with RA disease activity measures lacking CRP.
|
Table 1. Random-effects meta-analysis of the correlation of MBDA with composite RA disease activity measures |
|||||
|
|
N cohorts |
Pooled r |
95% CI |
Cochrane Q |
P value* |
|
MBDA |
|||||
|
CDAI |
4 |
0.38 |
0.19-0.56 |
12.36 |
0.006 |
|
SDAI |
3 |
0.51 |
0.29-0.73 |
11.34 |
0.003 |
|
ΔMBDA |
|||||
|
ΔDAS28-CRP |
3 |
0.51 |
0.38-0.64 |
1.67 |
0.44 |
|
*Significance of Cochrane Q test for heterogeneity |
|||||
To cite this abstract in AMA style:
Johnson T, Register KA, Schmidt C, O'Dell JR, Mikuls TR, Michaud K, England BR. Correlation of the Multi-Biomarker Disease Activity Score with Composite Rheumatoid Arthritis Disease Activity Measures: A Systematic Review and Meta-Analysis [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/correlation-of-the-multi-biomarker-disease-activity-score-with-composite-rheumatoid-arthritis-disease-activity-measures-a-systematic-review-and-meta-analysis/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/correlation-of-the-multi-biomarker-disease-activity-score-with-composite-rheumatoid-arthritis-disease-activity-measures-a-systematic-review-and-meta-analysis/