Session Information
Date: Sunday, October 26, 2025
Title: (0233–0279) Miscellaneous Rheumatic & Inflammatory Diseases Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Recurrent pericarditis (RP) is a chronic autoinflammatory disease (mediated by IL-1) that requires long-term treatment, and selection of therapy is guided by multiple factors. Cardiac magnetic resonance (CMR) imaging characterizes pericardial inflammation and may inform RP management. Rilonacept, an IL-1α and IL-1β cytokine trap, is the only FDA-approved treatment for RP. We analyzed all CMR use prior to rilonacept initiation in RESONANCE, a US observational RP registry.
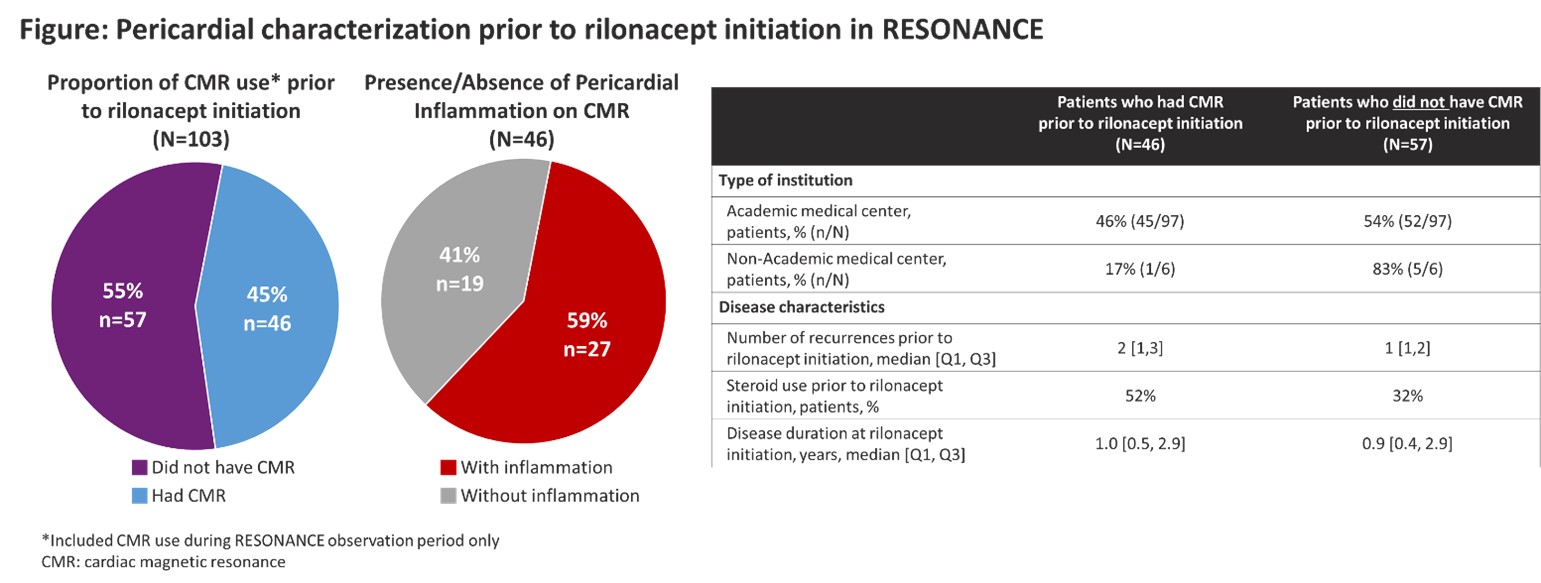
Methods: CMR use data were analyzed from 103 active pts at 22 sites (19 academic medical centers [AMCs], n=97; 3 non-AMC sites, n=6) who initiated rilonacept during RESONANCE up to Sep 9, 2024 (223.9 pt-yrs in median [Q1:Q3] 2.2 [1.4, 3.0] yrs).
Results: In 103 pts initiating rilonacept (mean [SD] age 49.7 [17.0] yrs, 56% female; median observation 0.8 [0.4, 1.0] yrs), median disease duration was 1.0 [0.4, 2.9] yr, with 1.5 [1, 2] prior recurrences. 45% (46/103) of pts had CMR before rilonacept initiation, 98% (45/46) of whom were managed at AMCs; 59% (27/46) showed pericardial inflammation. 54% (52/97) of rilonacept initiators at AMCs and 83% (5/6) at non-AMCs did not have CMR (Figure). Those having CMR had similar disease duration (1.0 [0.5,2.9] yr) but more prior recurrences (2 [1, 3]) and more prior steroid use (52%) than those not having CMR (0.9 [0.4, 2.9] yrs; 1 [1, 2]; 32%).
Conclusion: Recurrent pericarditis is a chronic disease that requires long-term treatment, and selection of therapy is guided by multiple factors. While CMR has utility amongst expert cardiologists in diagnosis, pericardial characterization, and monitoring, it was obtained in more clinically complex RP pts; real-world data indicate that pericardial imaging with CMR prior to rilonacept initiation was performed primarily at AMCs but in less than half of AMC patients (pericardial inflammation was present in approximately half); clinical criteria informed rilonacept initiation in the remainder.
To cite this abstract in AMA style:
Weber B, Cremer P, Garshick M, Luis S, Raisinghani A, Parameswaran V, Curtis A, Klein A, Paolini J. Contemporary Recurrent Pericarditis Management – Real-world Evidence of Limited Cardiac Magnetic Resonance Imaging Prior to Initiating Rilonacept [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/contemporary-recurrent-pericarditis-management-real-world-evidence-of-limited-cardiac-magnetic-resonance-imaging-prior-to-initiating-rilonacept/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/contemporary-recurrent-pericarditis-management-real-world-evidence-of-limited-cardiac-magnetic-resonance-imaging-prior-to-initiating-rilonacept/