Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Lupus nephritis (LN) is associated with excess morbidity and mortality, with prior studies finding a disproportionate impact on Black patients. We sought to determine the patterns of treatment and healthcare utilization and the burden of kidney and non-kidney adverse health outcomes in a large, contemporary United States lupus inception cohort.
Methods: We identified a systemic lupus erythematosus (SLE) inception cohort from TriNetX, an electronic health record (EHR) database with patients from academic and non-academic medical centers across the United States. We included patients with SLE (≥2 ICD codes ≥30 days and ≤2 years apart) between January 2005 and August 2021 with at least 5 years of enrollment prior to the first ICD code. We identified patients with LN, defined as ≥2 specific nephritis codes or ≥1 nephritis code and a kidney biopsy. Patients were followed until the end of the study period, death, or disenrollment from the database. We assessed kidney and non-kidney health outcomes, including CKD stage ≥3, end-stage kidney disease (ESKD), and major adverse cardiac events (MACE) according to sex and race/ethnicity over 2 years (primary) using multivariable logistic regression. We also assessed LN treatment and healthcare utilization patterns.
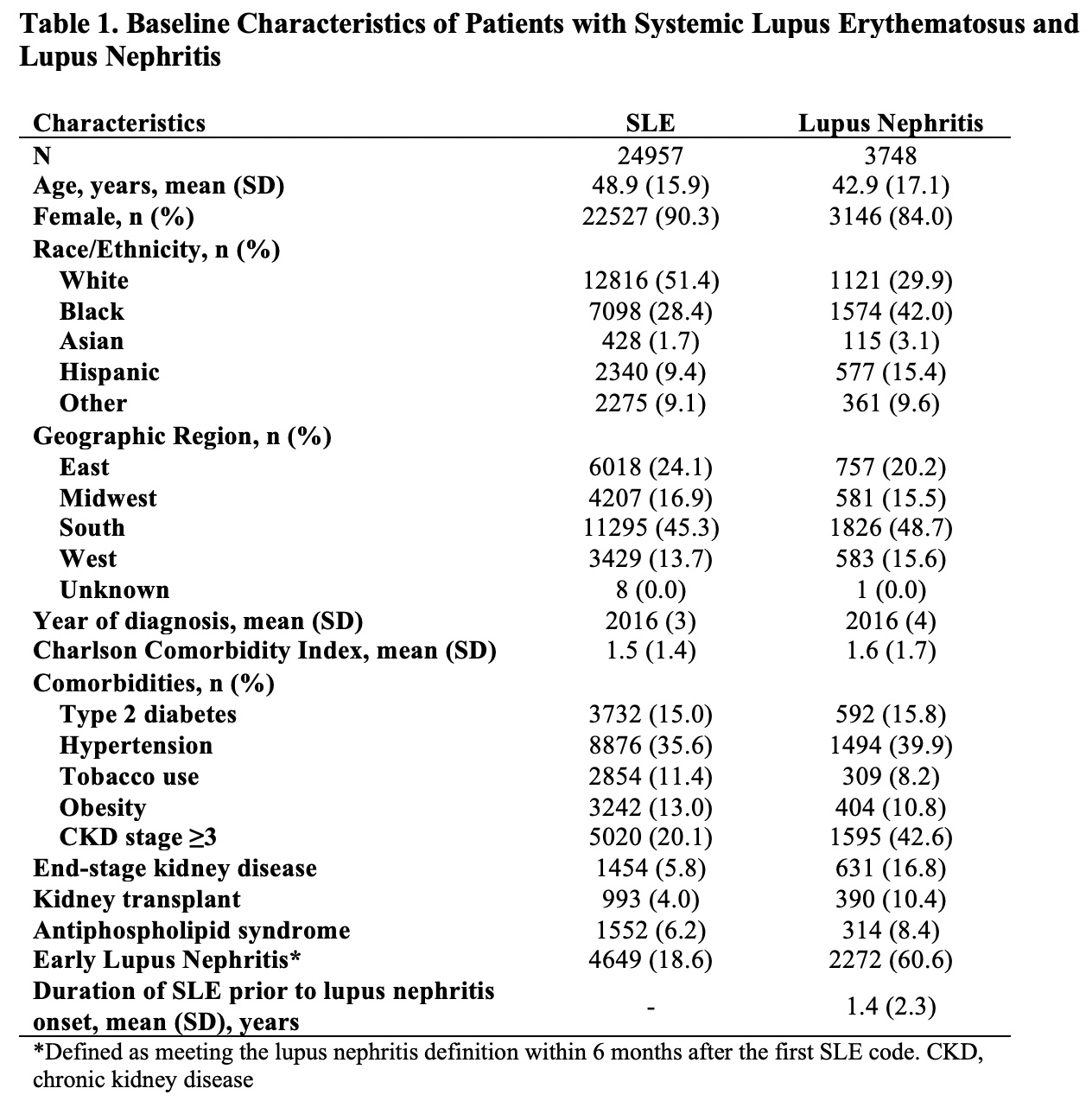
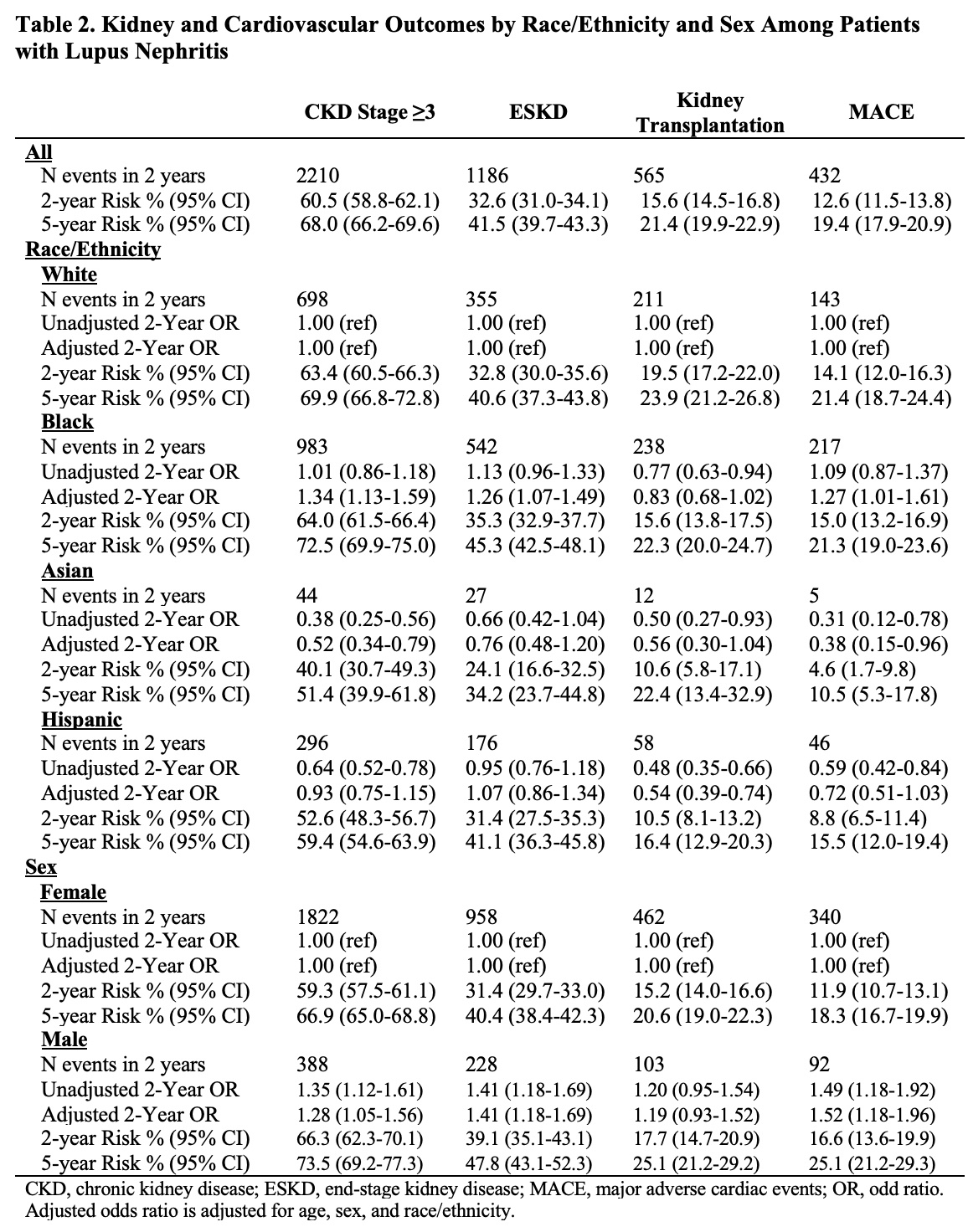
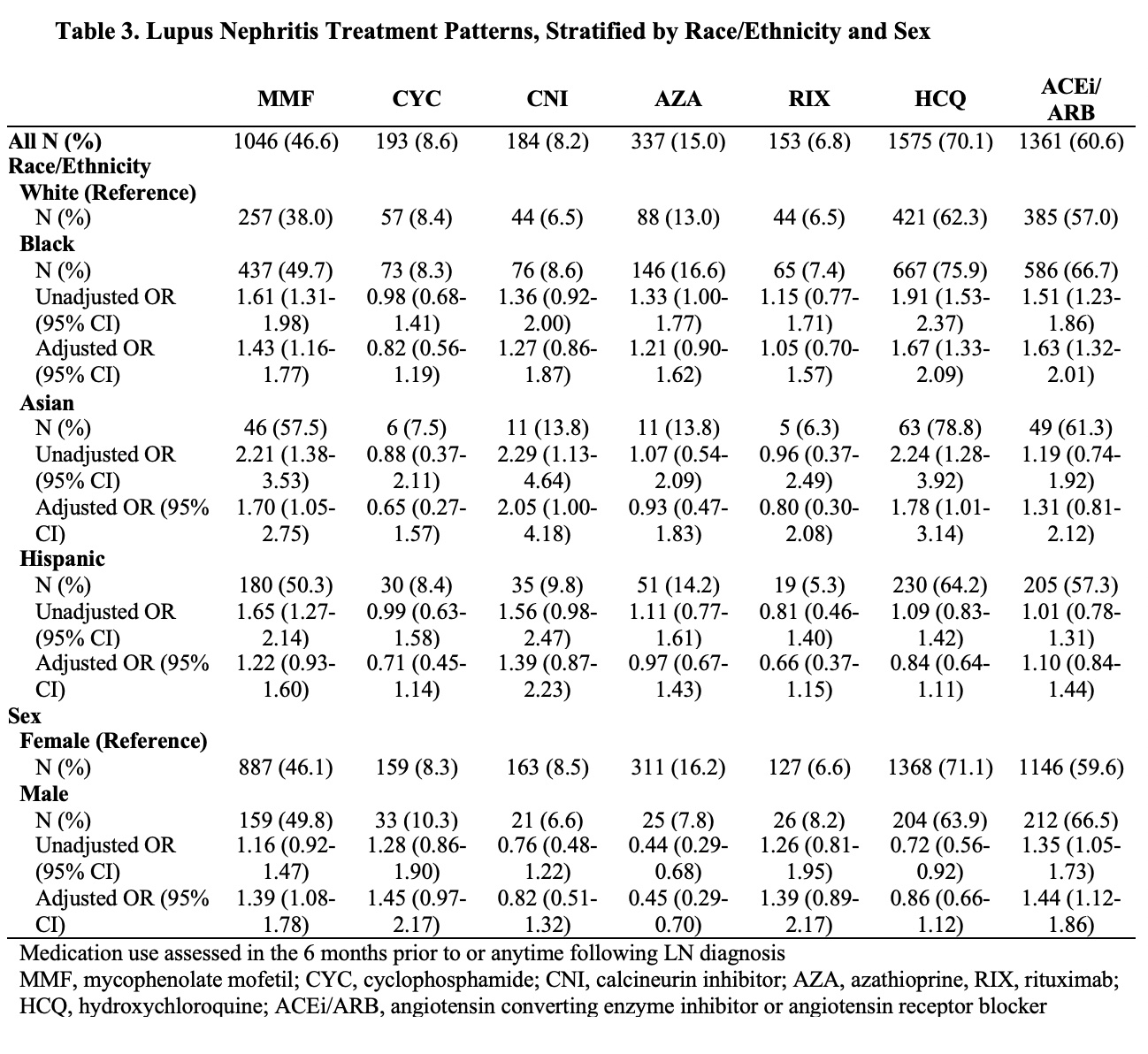
Results: There were 24,957 SLE patients in the inception cohort, of which 3748 (15%) had LN (Table 1). Patients with LN were younger at onset (42.9 vs 48.9 years) and more commonly Black (42 vs 28%) or Hispanic (15 vs 9%) than overall SLE patients. The 5-year risks of CKD stage ≥3 and ESKD among patients with LN were 68% and 42%, respectively; the risk of ESKD was higher among Black than White individuals with LN (adjusted OR [aOR] for ESKD 1.26 [95% CI 1.07-1.49]; Table 2). Additionally, 21% of LN patients received a kidney transplant within 5 years of LN onset, after a mean of 3.1 years (SD 3.1) from LN-ESKD onset. Black patients had a higher risk of MACE than White patients (aOR 1.27 [95% CI 1.01-1.61]. Males with LN had higher rates of ESKD and MACE than females. Mycophenolate, hydroxychloroquine, and angiotensin converting enzyme inhibitor/angiotensin receptor blockers were used by 47%, 70%, and 61% of patients with LN, respectively (Table 3). Mycophenolate was more often used by Black (aOR 1.43 [95% CI 1.16-1.77]) and Asian (aOR 1.70 [95% CI 1.05-2.75]) than White patients with LN. Black patients were more likely than White patients to use glucocorticoids at two years following LN diagnosis (aOR 1.40 [95% CI 1.12-1.75]). Black and Hispanic patients had more frequent ER/inpatient visits than White or Asian patients in the two years after LN onset (mean [SD] 3.5 [7.0] and 3.2 [7.2] vs. 2.5 [5.4] and 2.4 [9.2], respectively, with p< 0.01).
Conclusion: In this large EHR-based inception cohort of patients with SLE and LN, we observed a considerable risk of ESKD. Black patients had a higher risk of adverse kidney outcomes and MACE and were more frequently on prolonged glucocorticoids while experiencing frequent ER/inpatient visits. Males with LN had worse outcomes than females. These findings highlight the need for strategies to improve LN outcomes.
To cite this abstract in AMA style:
Patel A, Zhou B, Choi H, Jorge A. Contemporary Lupus Nephritis Treatment and Outcomes Among Patients with Systemic Lupus Erythematosus in the United States [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/contemporary-lupus-nephritis-treatment-and-outcomes-among-patients-with-systemic-lupus-erythematosus-in-the-united-states/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/contemporary-lupus-nephritis-treatment-and-outcomes-among-patients-with-systemic-lupus-erythematosus-in-the-united-states/