Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: HAQ-Di is broadly used to measure disability in RA, its assessment might influence taking decision process. However, it cannot differentiate disability related to arthritis, accrual damage, age, personal behaviors or comorbidities. We aimed to determine factors related to disability in a non-rheumatic population and evaluate its contributing factors.
Methods: We ask outpatients attendees of clinical specialties or first contact physician to fill out the HAQ-Di and have and structured interview during their scheduled visit. Those older than 18 years who signed informed consent were included. Participants with any musculoskeletal disease, chronic pain, neurological or psychiatric condition, use of drugs that impaired mobility or mental status, as well as illness in terminal stage were excluded. Demographic variables, formal education, exercise, and the Charlson index were recorded. Pearson’s correlation, chi square, Mann-Whitney-U or t-test were performed as appropriate. Contribution of each factor to the predicted disability was determined by forward stepwise multivariate regression modelling.
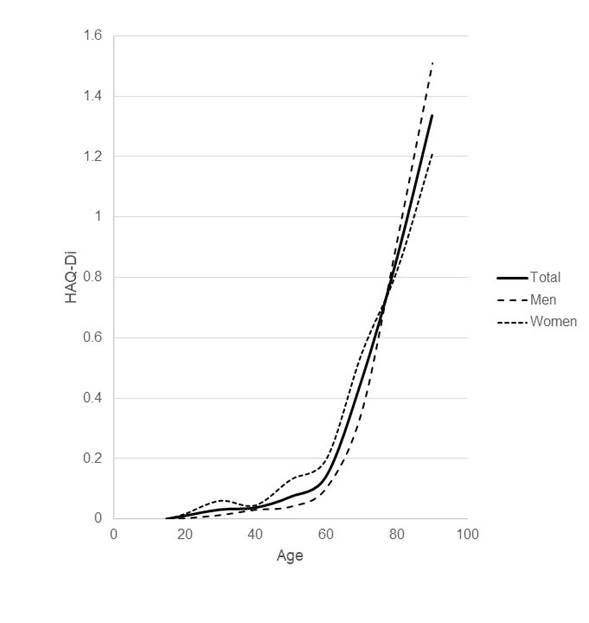
Results: A total of 1,506 subjects were included, their mean age was 54.7±15.8 years, 17% were younger than 40 years, 65% between 40 and 70 years, and 18% older than 70 years. One fourth were ever smokers, 40.7% female, BMI was 27.1±4.4 Kg/m2, Charlson index 1.5±1.7, HAQ-Di was 0.17±0.45 for the whole population; 25.1% declared some disability (HAQ-Di value >0). HAQ-Di values above 0.1 started at the 55 years subjects and increase to 1.3 at 90 years; it was higher in women than in men (0.25±0.54 versus 0.12±0.37; p <0.001). HAQ-Di showed correlation with age r=0.47 (p<0.001), and Charlson index, r=0.52 (p<0.001). Subjects with less than 10 years of formal education had a higher HAQ-Di, 0.52±0.73, compared with those with >10 years, 0.09±0.3 (p<0.001). Those who practice exercise on daily basis had a HAQ-Di of 0.09±0.32, those who did not any exercise had 0.45±0.69 (p<0.001). A regression model including standardized age (mean age value=0.17), sex (1=man), diagnosis of hypertension (1=yes) and diabetes (1=yes) explained the 25% of the HAQ-Di and predicted a HAQ score of 0.45.
Conclusion: One fourth of outpatients attending a general Hospital had disability. The main determinant is the age, but there is a significant contribution of comorbidity, high blood pressure and diabetes. Moreover, those who practice exercise on daily basis and those with higher education had the lowest HAQ-Di scores. We suggest that when HAQ-Di must be used in the RA population, they must be adjusted by age, sex and comorbidity.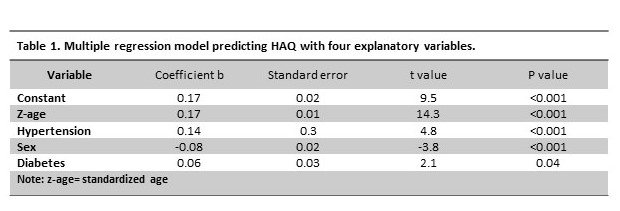
To cite this abstract in AMA style:
Arce-Salinas CA, ESPINOSA-ORTEGA HF, Enriquez-Antonio O. Components of Impaired Physical Function and Disability in a Non-Rheumatic Population. Normative Values of the Health Assessment Questionnaire Disability Index [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/components-of-impaired-physical-function-and-disability-in-a-non-rheumatic-population-normative-values-of-the-health-assessment-questionnaire-disability-index/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/components-of-impaired-physical-function-and-disability-in-a-non-rheumatic-population-normative-values-of-the-health-assessment-questionnaire-disability-index/