Session Information
Date: Saturday, November 16, 2024
Title: Abstracts: Miscellaneous Rheumatic & Inflammatory Diseases I
Session Type: Abstract Session
Session Time: 3:00PM-4:30PM
Background/Purpose: No studies to date have evaluated the comparative efficacy of disease modifying antirheumatic drugs (DMARDs) for cardiac sarcoidosis.
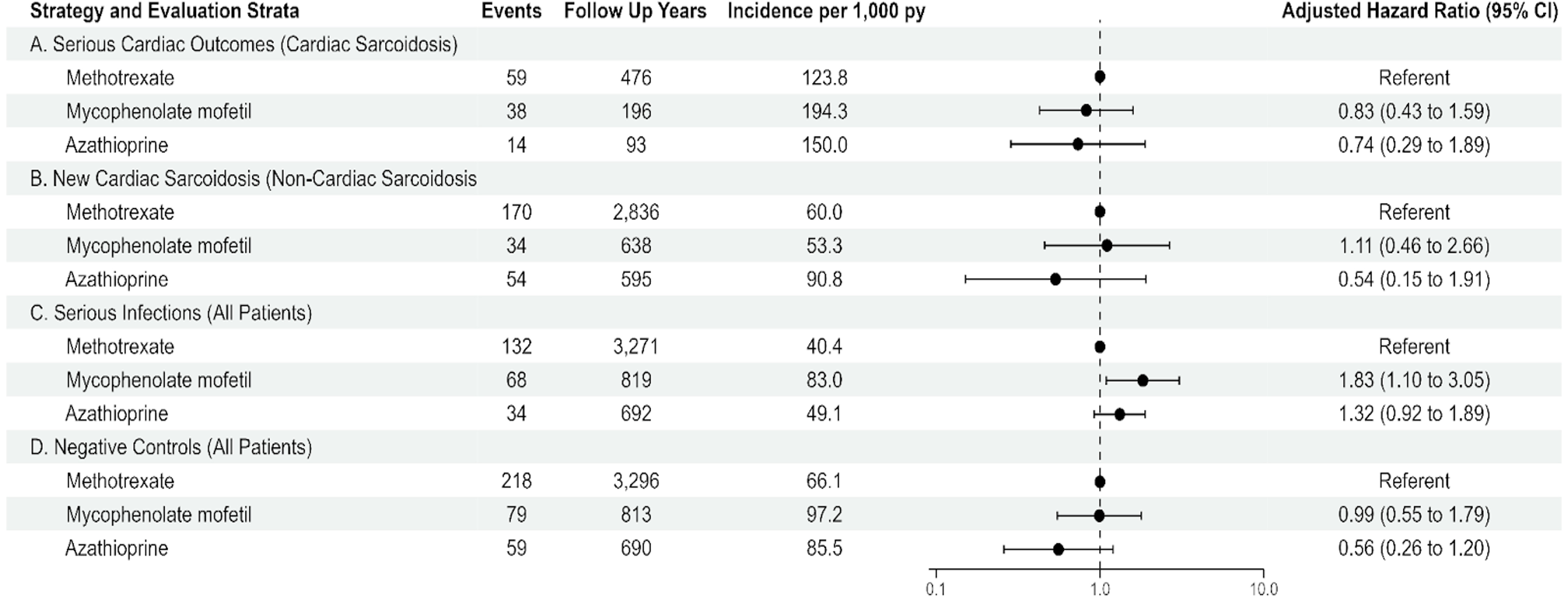
Methods: We performed a retrospective cohort study of new users of methotrexate, mycophenolate, or azathioprine for sarcoidosis using the US-based TriNetX electronic health records database from 2008-2023. Patients were stratified by whether they had cardiac sarcoidosis at baseline (defined by atrioventricular block, ventricular block, ventricular arrhythmia, heart failure, or sarcoid myocarditis one year prior or 90 days after the index date). The primary outcome of interest was incident cardiac sarcoidosis for the non-cardiac sarcoidosis cohort or having a severe cardiac outcome (pacemaker or defibrillator insertion, cardiac arrest, cardiac transplantation, or death) for the cardiac sarcoidosis group. The unadjusted rate of events was presented as incident rate ratios (IRR) and adjusted hazard ratios (HR) were calculated using weighted Cox proportional hazards regressions for each cohort. The risk of serious infectious adverse events and negative control outcomes (osteoarthritis, injury, trauma) were also evaluated.
Results: Among 3,441 patients with sarcoidosis, 601 were defined as cardiac sarcoidosis and 2,840 as non-cardiac sarcoidosis. The average age of the cohort was 52.1 years (standard deviation 11.9 years) and the majority were female (55.9%) and white (50.0%). Among patients with cardiac sarcoidosis at baseline, the risk of serious cardiac outcomes was similar for patients who initiated therapy with mycophenolate mofetil (aHR 0.83, 95% CI 0.43-1.59) or azathioprine (aHR 0.74, 95% CI 0.29-1.89) as compared to methotrexate. Among patients who did not have cardiac sarcoidosis at baseline, the risk of developing cardiac sarcoidosis was similar for patients who initiated therapy with mycophenolate mofetil (aHR 1.11, 95% CI 0.46-2.66) and azathioprine (aHR 0.54, 95% CI 0.15-1.91) as compared to methotrexate. Serious infections were more common among patients who initiated mycophenolate mofetil (aHR 1.83, 95% CI 1.10-3.05) and numerically elevated for azathioprine (aHR 1.32, 95% CI 0.92-1.89).
Conclusion: Treatment strategies did not significantly change the risk of serious cardiac outcomes among patients with cardiac sarcoidosis or the risk of incident cardiac sarcoidosis among patients who did not have cardiac involvement at baseline. Methotrexate had a favorable safety profile as compared to mycophenolate mofetil or azathioprine.
Abbreviations: person years (py), confidence interval (CI), patients (pts), disease (dx), tumor necrosis factor inhibitor (TNF)
To cite this abstract in AMA style:
Putman M, Brooks L, Kivlin W, Mohananey D, Sabchyshyn V. Comparative Effectiveness of Disease Modifying Antirheumatic Drugs for Cardiac Sarcoidosis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/comparative-effectiveness-of-disease-modifying-antirheumatic-drugs-for-cardiac-sarcoidosis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/comparative-effectiveness-of-disease-modifying-antirheumatic-drugs-for-cardiac-sarcoidosis/