Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Scleroderma renal crisis (SRC) is a life-threatening complication of systemic sclerosis (SSc), historically described to occur within the first 5 years of SSc diagnosis. However, it has been observed by clinicians to occur beyond 5 years. The characteristics of the population with late onset SRC have not been studied. In this analysis, we aim to describe the prevalence, clinical features and outcomes of late onset SRC and compare them to early onset SRC.
Methods: This retrospective study included patients diagnosed with SRC between 1995 to 2018 at three university-affiliated hospitals. Late onset SRC was defined as SRC occurring 5 years after the initial SSc symptoms. After obtaining IRB approval, data was extracted that included demographics, SRC onset, clinical characteristics, laboratory data, and outcomes (hemodialysis and mortality).
Continuous data were expressed as mean ± standard deviation or median (interquartile range), while categorical as frequencies and percentages. Differences were analyzed via Pearson’s chi-square or Fisher’s exact test. Statistical significance was set at p < 0.05, analyzed using Minitab (v19) and R (4.3.0).
Results: A total of 223 SRC patients were identified, with 169 (75.8%) classified as early onset and 54 (24.2%) as late onset. Early onset SRC typically developed within the first year of SSc symptoms, while late onset had a mean SRC onset at 12.2 years after SSc symptoms.
No significant differences were found in age and race between the two groups; however, interestingly male predominance was observed in late onset SRC as compared to early onset SRC (59% vs 9%; p < 0.001). There were no differences in comorbidities except preceding hypertension which was more prevalent in early onset (11%) compared to late onset (2%) with p = 0.05. Steroid exposure was more common in late onset SRC (56%) compared to early onset (29%) with p = 0.04, as were overlap syndromes (64% vs 32%; p = 0.03). Cardiac involvement (38% vs 14%) was more common in early group compared to late onset (p = 0.01). No significant differences were found in other organ manifestations of SSc (Table 1).
There was no significant difference in autoantibodies between early and late onset SRC (Table 2).
No significant differences were observed between the two groups in renal outcomes, including the need for hemodialysis at SRC diagnosis and one-year, as well as long term outcomes indicated by 1 year and 5 year mortality rates (table 3).
Conclusion: 24% of our 223 SRC patients had late onset of SRC, a median of 10 years after the onset of disease. Males were significantly more likely to have late onset compared to early onset, however, otherwise patients with late onset had similar outcomes in terms of hemodialysis requirement and mortality as the early onset patients. Our findings reveal comparable clinical characteristics and outcomes between early and late onset SRC, underlying the importance of recognizing SRC regardless of disease duration to optimize outcomes.
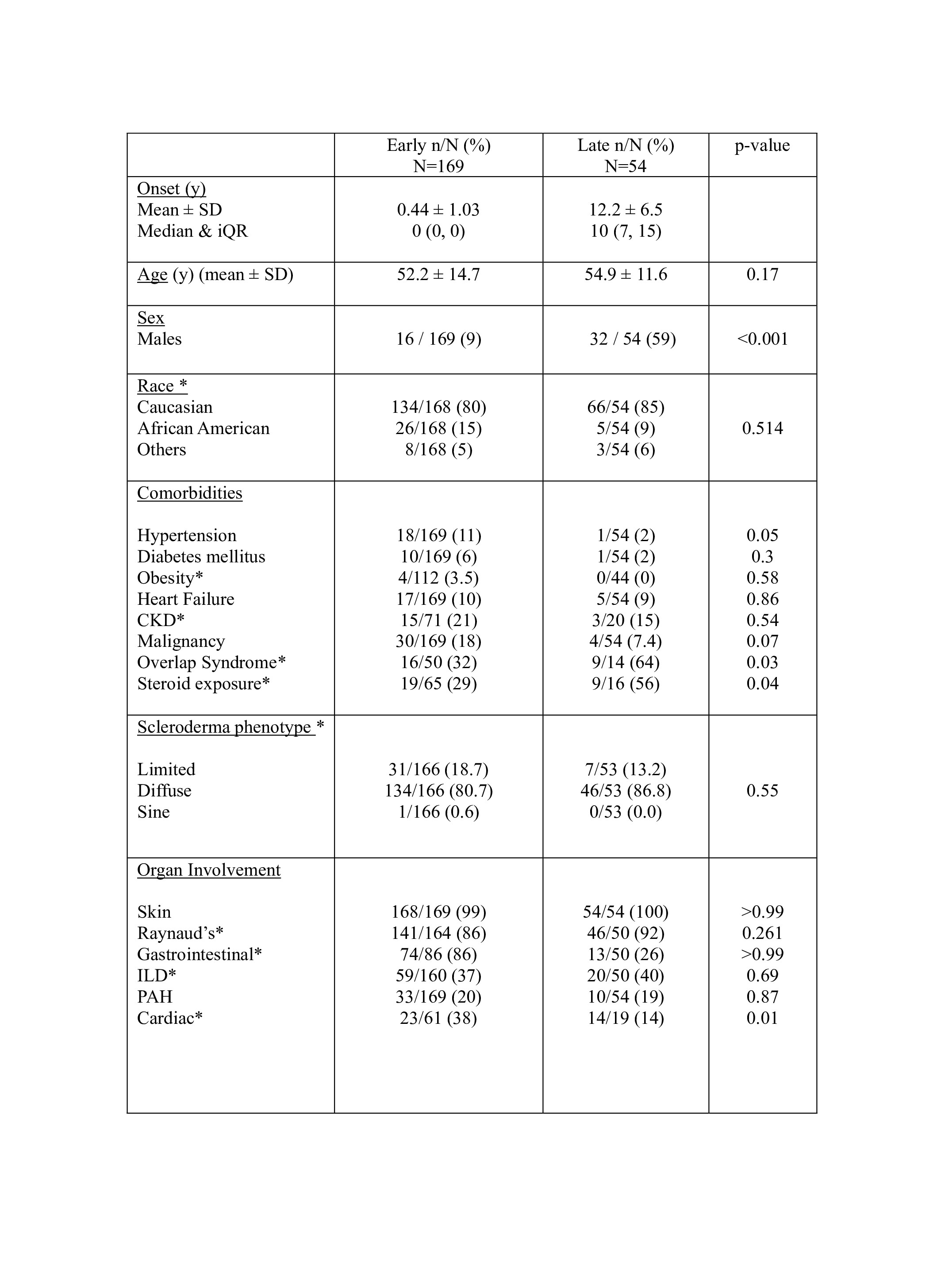
(Y: years, SD: standard deviation, iQR: interquartile range, CKD: chronic kidney disease III or above, ILD: Interstitial Lung Disease, PAH: Pulmonary Arterial Hypertension, overlap syndrome: Scleroderma with Sjogren’s syndrome, Polymyositis, lupus, Rheumatoid arthritis, *: missing data)
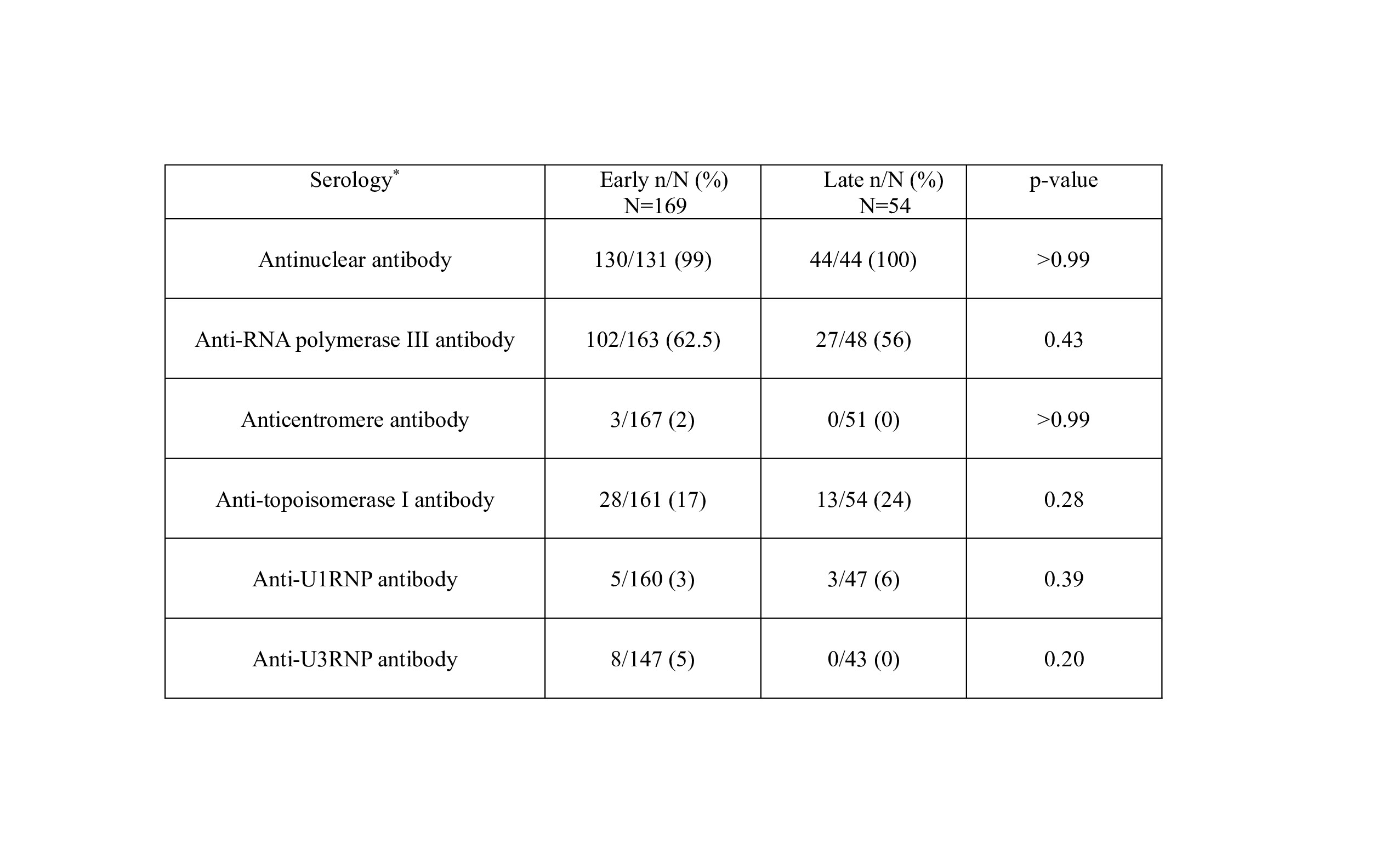
(abbreviations: RNP: ribonucleoprotein, *: Missing data)
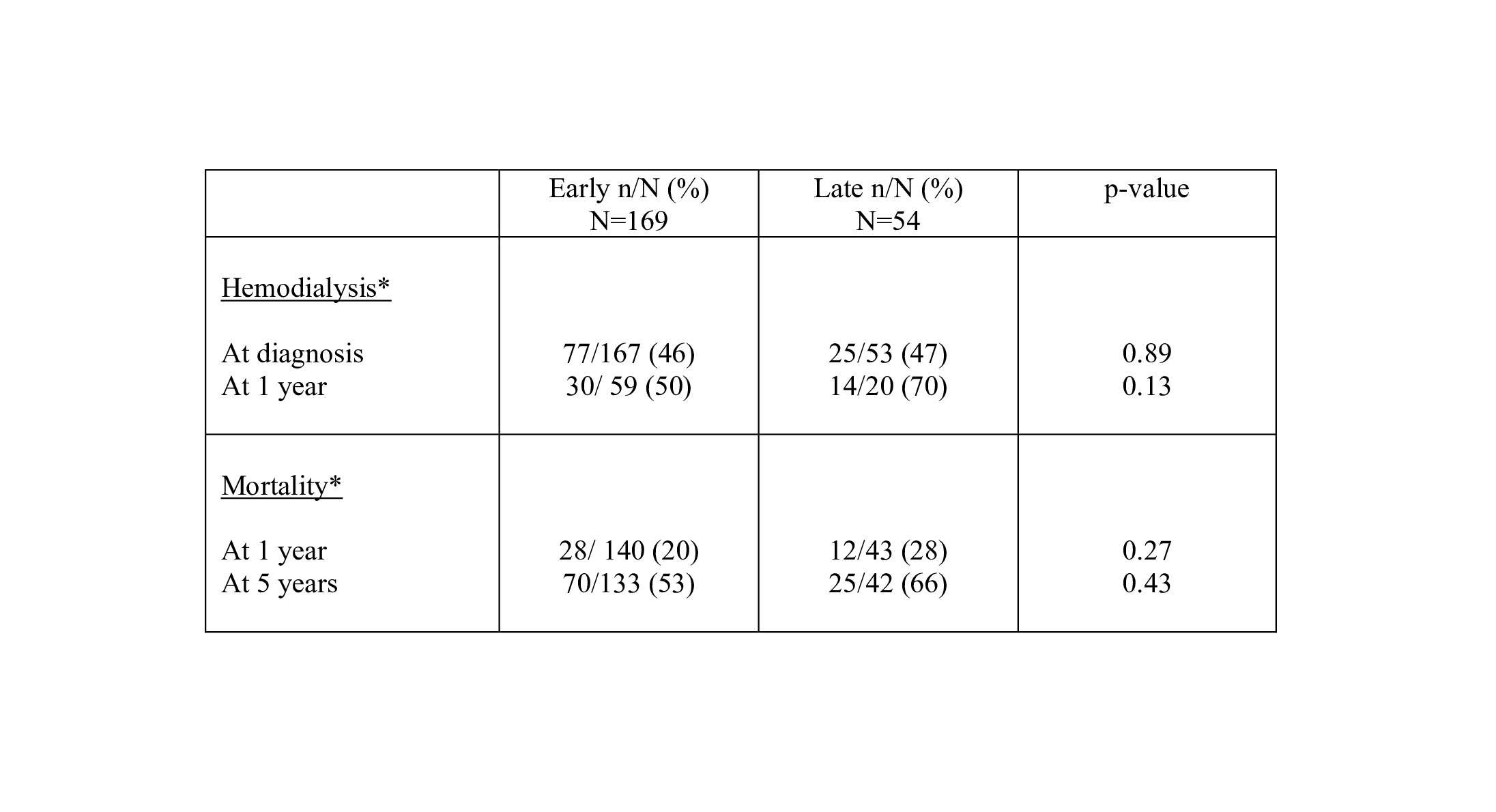
(*: missing data)
To cite this abstract in AMA style:
Wajid S, Shapiro L, Steen V, Domsic R, Feustel P, Mehta S. Comparative Analysis of Clinical Features and Outcomes in Late Onset vs. Early Onset Scleroderma Renal Crisis – A Multicenter Study [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/comparative-analysis-of-clinical-features-and-outcomes-in-late-onset-vs-early-onset-scleroderma-renal-crisis-a-multicenter-study/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/comparative-analysis-of-clinical-features-and-outcomes-in-late-onset-vs-early-onset-scleroderma-renal-crisis-a-multicenter-study/