Session Information
Date: Monday, November 18, 2024
Title: Muscle Biology, Myositis & Myopathies – Basic & Clinical Science Poster III
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Immune cell profiling plays a pivotal role in the pathogenesis of idiopathic inflammatory myopathy (IIM). Characterizing immune cell subtypes, such as CD4+ T cells, CD8+ T cells, CD19+ B cells, natural killer (NK) cells, is essential for understanding the immunopathogenesis and treatment of these disorders. Immune cells contribute to aberrant immune responses, impacting disease progression. This nuanced understanding forms the basis for investigating targeted interventions to modulate specific immune cell populations and improve outcomes in patients with IIM.
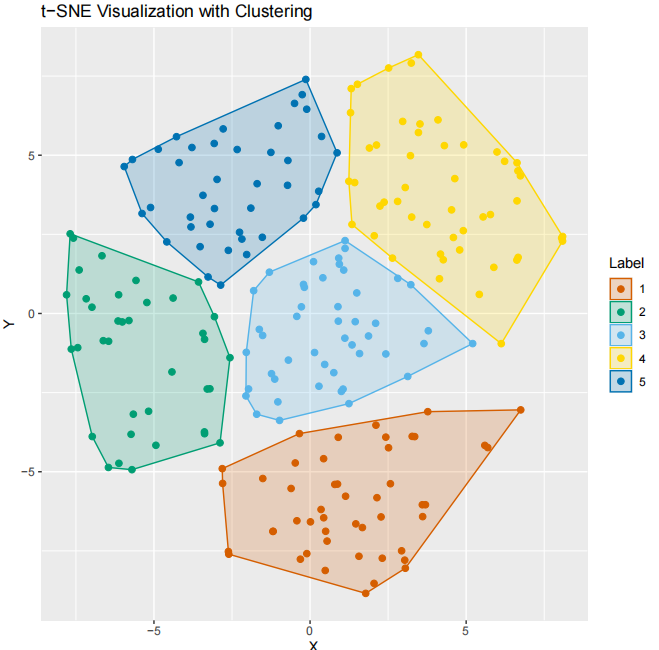
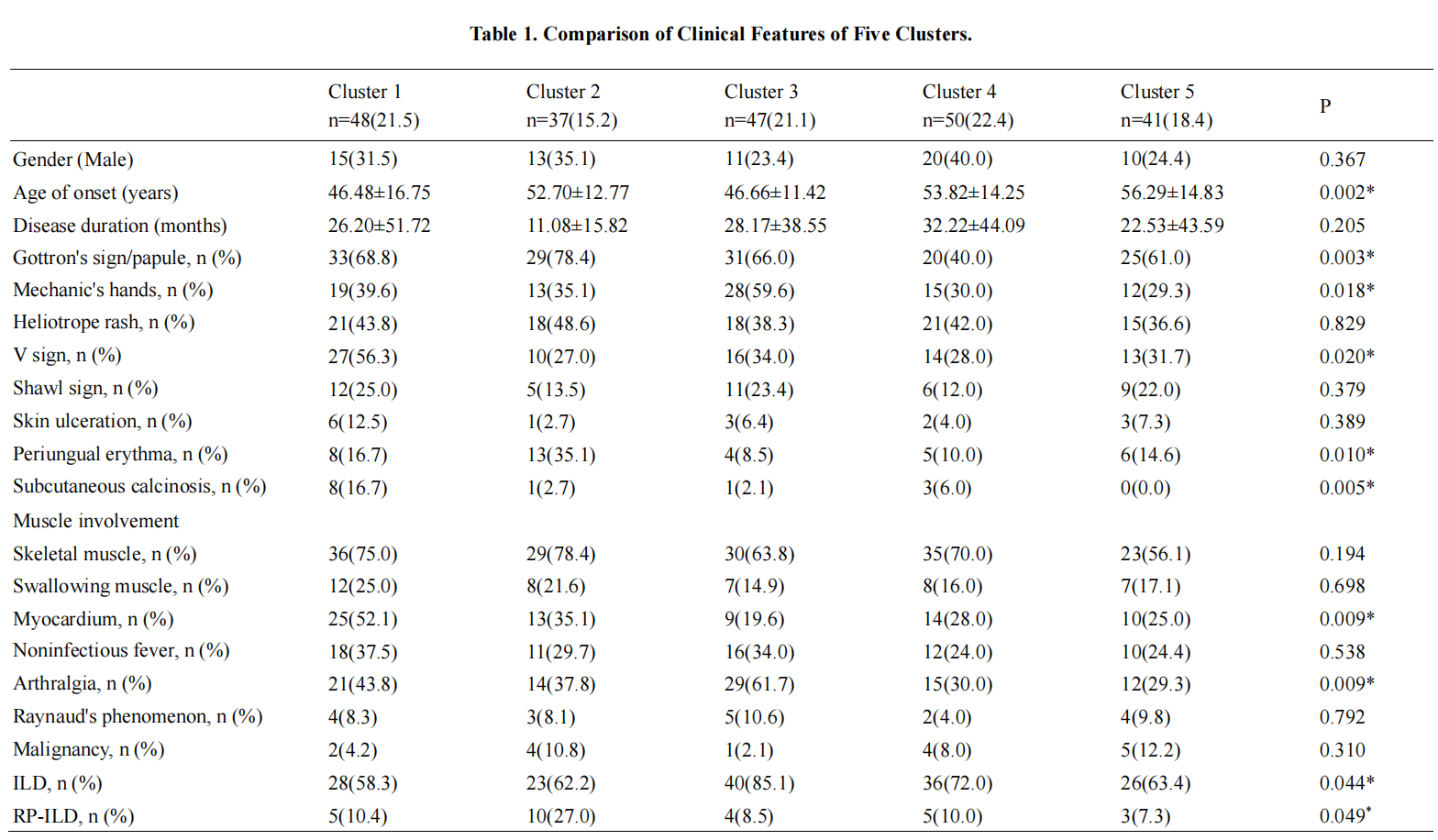
Methods: Data from 223 patients in a retrospective cohort of IIM at Peking University People’s Hospital from 2012 to 2023 were analyzed. Cluster heatmap and t-distributed Stochastic Neighborhood Embedding (t-SNE) were employed using patient-reported outcomes, encompassing total lymphocyte count, CD3+ T cells, CD4+ T cells, CD8+ T cells, CD19+ B cells, and NK cells. Elbow method was used to select the optimal number of clusters and described each cluster according to Clinical and laboratory differences (mean and proportions). The therapeutic effects of tofacitinib and low-dose Interleukin-2 were evaluated in conjunction with this analysis.
Results: Based on immune cell subpopulations, these patients are categorized into five groups. Group 1 shows elevated proportions of CD4+ T cells and Naïve Th cells, with a higher incidence of V-sign, subcutaneous calcification, and myocardial involvement. Group 2 patients exhibit a lower proportion of CD3+ T cells, higher CD19+ B cell ratio, and an increased occurrence of Gottron’s sign, periungual erythema, and rapidly progressive interstitial lung disease (RP-ILD) compared to other groups. Group 3 patients have a higher proportion of CLA+ Treg cells, often presenting with mechanic’s hands, arthritis, and ILD. Group 4 patients have higher proportions of CD8+ T cells and TNFα+ CD4+ T cells, with a higher prevalence of immune-mediated necrotizing myopathy. Group 5 patients have higher proportions of NK cells, and overall, exhibit milder symptoms. Regarding treatment, groups 1, 3, and 4 show positive responses to tofacitinib, while some patients in groups 2 and 5 demonstrate poor response to tofacitinib treatment. Moreover, some patients in groups 1 and 3 exhibit a poor response to low-dose interleukin-2, while patients in groups 2, 4, and 5 respond well to low-dose interleukin-2 treatment.
Conclusion: Immune cell subpopulation clustering analysis in IIM patients reveals distinctive features associated with diverse clinical manifestations. Each patient group exhibits varying responses to different treatment strategies, providing valuable insights for guiding the management and prognosis of IIM.
To cite this abstract in AMA style:
xing x, Li Y, He J. Clustering Analysis of Immune Cell Subtypes and Clinical Phenotypes in Idiopathic Inflammatory Myopathy [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/clustering-analysis-of-immune-cell-subtypes-and-clinical-phenotypes-in-idiopathic-inflammatory-myopathy/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clustering-analysis-of-immune-cell-subtypes-and-clinical-phenotypes-in-idiopathic-inflammatory-myopathy/