Session Information
Session Type: Poster Session B
Session Time: 8:30AM-10:30AM
Background/Purpose: The Idiopathic Inflammatory Myopathies (IIM) are often difficult to treat, require chronic steroid therapy, and can remain active despite multiple treatment regimens. The objective of this study is to identify clinical characteristics at time of diagnosis and follow on treatment strategies which have prognostic value related to disease outcomes.
Methods: We performed a retrospective chart review of patients diagnosed with an inflammatory myopathy within the Department of Defense (DoD) between January 2006 and December 2020. Identified by the ICD-10 diagnosis codes for inflammatory myositis, patients were included if diagnosed at one of fifteen hospitals within the DoD. All patients met either the Bohan and Peter 1975 or EULAR/ACR classification criteria for definite or probable myositis. Demographic and laboratory data were identified at initial presentation. Myositis complications and treatment regimens were collected during the follow up period. Clinical outcomes were based on the most recent evaluation. Patients were categorized into one of five clinical outcome groups. We used ANOVA modeling to identify significant parameters and performed Chi square tests for categorical variables and Student’s t-tests for continuous variables within groups.
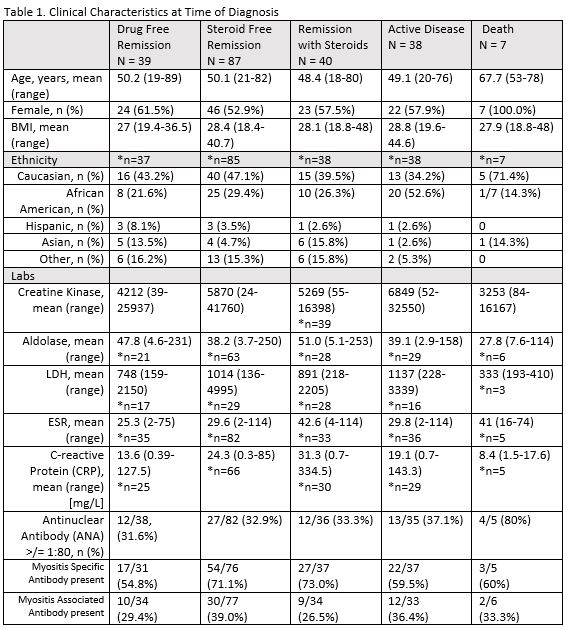
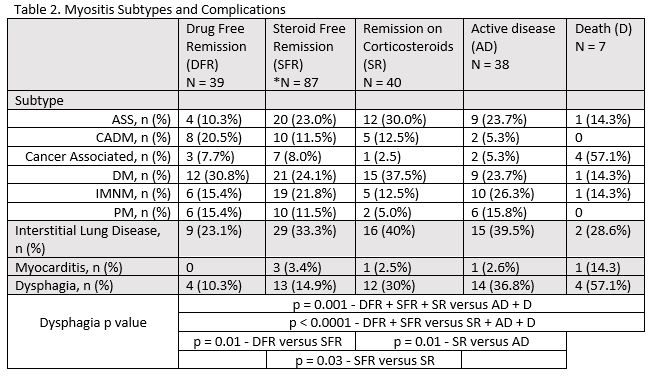
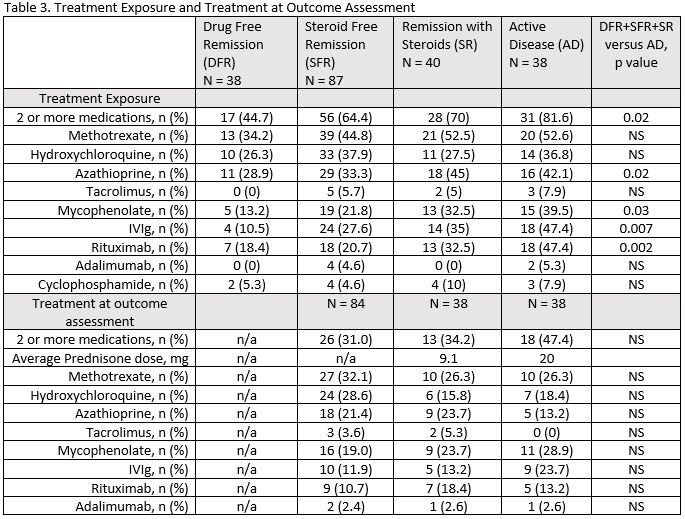
Results: Two hundred and eleven patients were followed between 2 and 180 months. Steroid free remission was achieved in 126 (59.7%) of which 39 (18.5%) achieved drug free remission. Thirty-eight patients (18.0%) remained with clinically active disease at end of study. African American ethnicity was associated with persistent disease activity (p< 0.001) (Table 1). There was no significant outcome associations for the subtypes of IIM, age, gender, and BMI. ESR was significantly lower in patients reaching steroid free remission compared to remission with steroids (p=0.016), but not with the active disease cohort. No other laboratory values correlated with outcomes. Dysphagia, but not interstitial lung disease or myocarditis, was associated with worse disease outcomes (Table 2). Patients who achieved any form of disease remission were more likely to see a 90% reduction in creatine kinase (CK) levels at 12 months of therapy than those with active disease (OR 2.7, CI 1.1 – 6.5). There was a trend with CK reduction of 87% at 3 months and end of study remission (OR 2.29, CI 0.99 – 5.24). Treatment regimens at final assessment did not correlate with specific outcomes, but historical exposure to second line agents mycophenolate (p=0.03), azathioprine (p=0.008), intravenous immunoglobulin (IVIg) (p=0.007) or rituximab (p=0.002) was associated with active disease (Table 3).
Conclusion: Steroid free remission was achieved in nearly 60% of the IIM population, but chronic steroid exposure and poor clinical outcomes were still common. African American ethnicity, dysphagia, and second line therapies were all associated with worse outcomes, identifying a need for more effective treatments strategies. Creatine kinase at time of onset did not correlate with outcomes, but a dramatic drop ( >90% at 12 months) may have prognostic implications for remission, suggesting a need for a treat to target strategy.
To cite this abstract in AMA style:
Mecham D, Moore W, Ward I. Clinical Outcomes in Idiopathic Inflammatory Myositis Within the Military Health System: A 15 Year Retrospective Review [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/clinical-outcomes-in-idiopathic-inflammatory-myositis-within-the-military-health-system-a-15-year-retrospective-review/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-outcomes-in-idiopathic-inflammatory-myositis-within-the-military-health-system-a-15-year-retrospective-review/