Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: To describe the clinical profile and predictors of mortality of AAV patients in Hong Kong. To compare the accuracy of the latest Five-factor Score (FFS-2009) and the Birmingham Vasculitis Activity Score (BVAS) in prediction of survival with this local cohort.
Methods: A retrospective observational study on newly diagnosed AAV patients, from 1st January 2011 to 31st March 2022, managed in the Kowloon West Cluster (KWC) hospitals in Hong Kong. Demographic and baseline characteristics, clinical profile, and treatment profile were reviewed. Factors associated with mortality were analysed with Cox proportional hazards model. The performances of FFS and BVAS in mortality prediction were analysed by Receiver Operating Characteristic (ROC) curves.
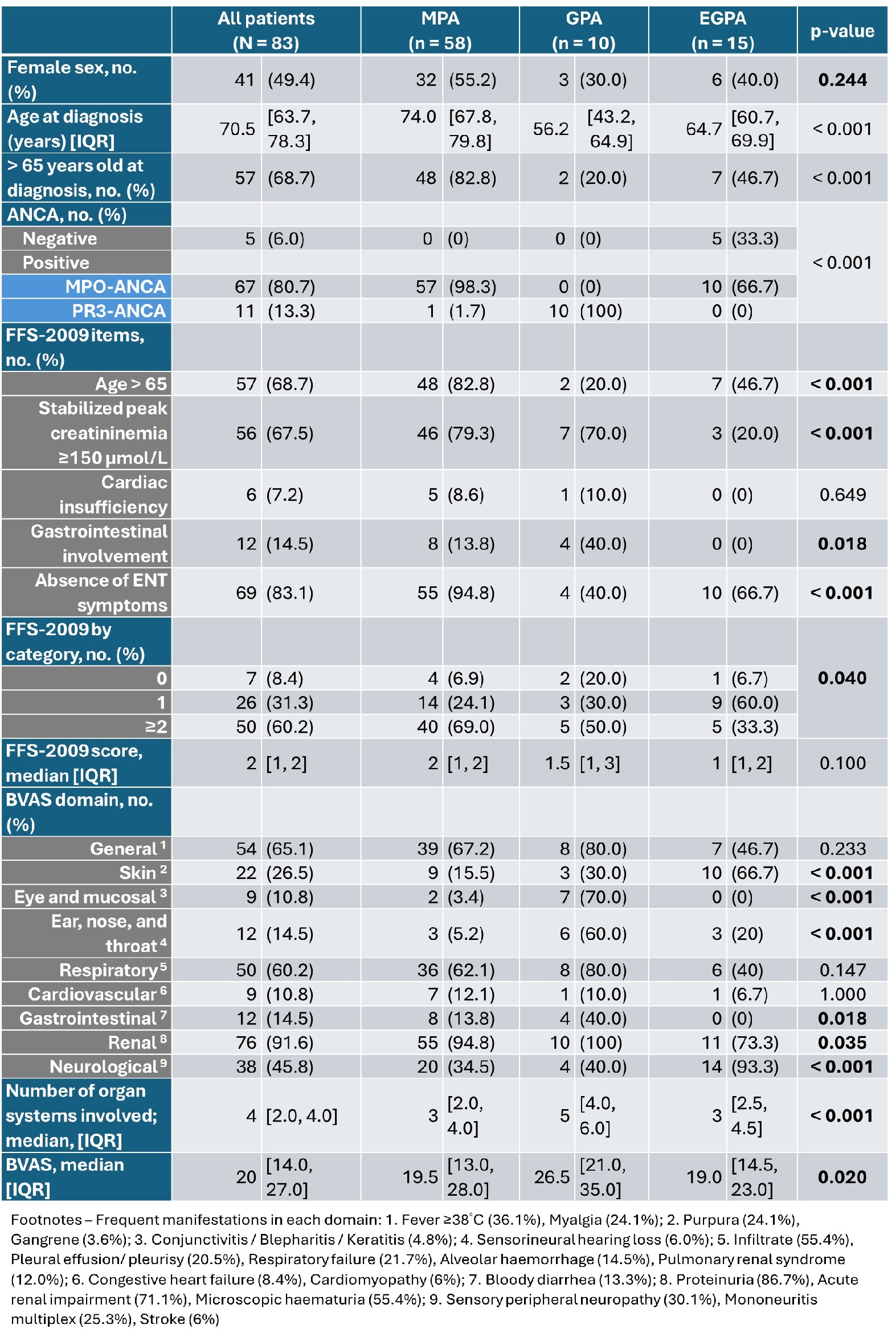
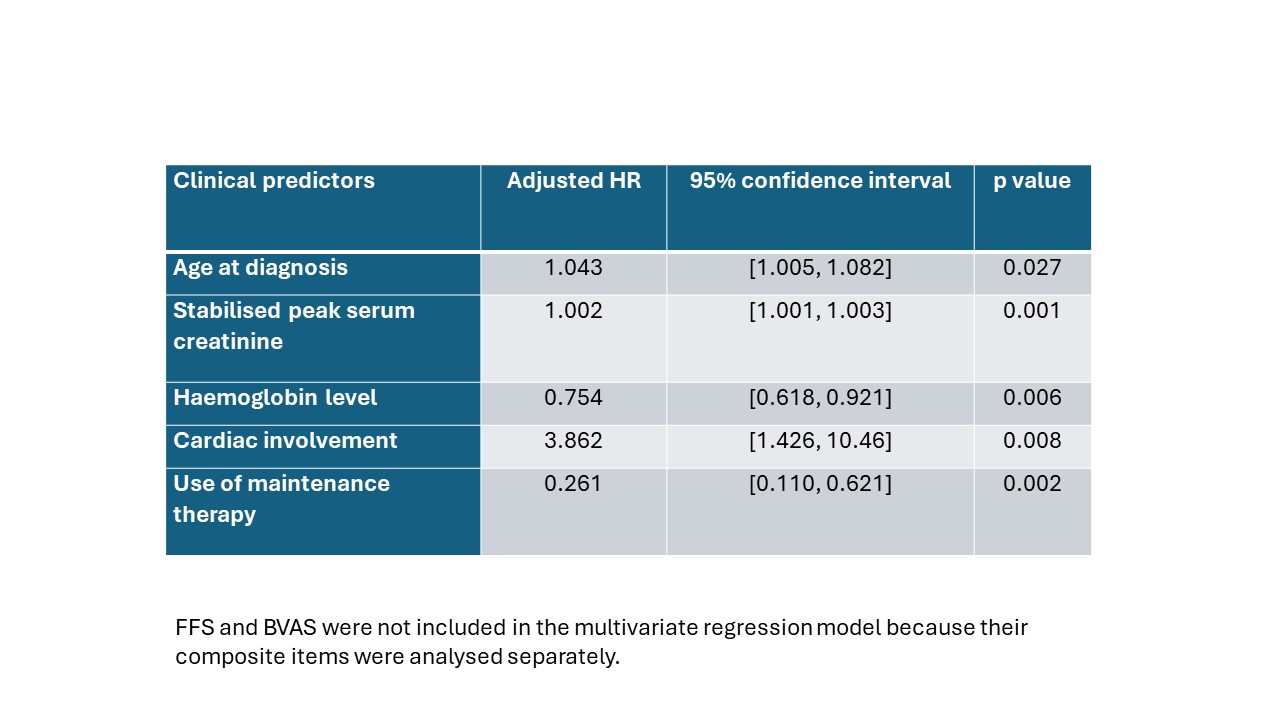
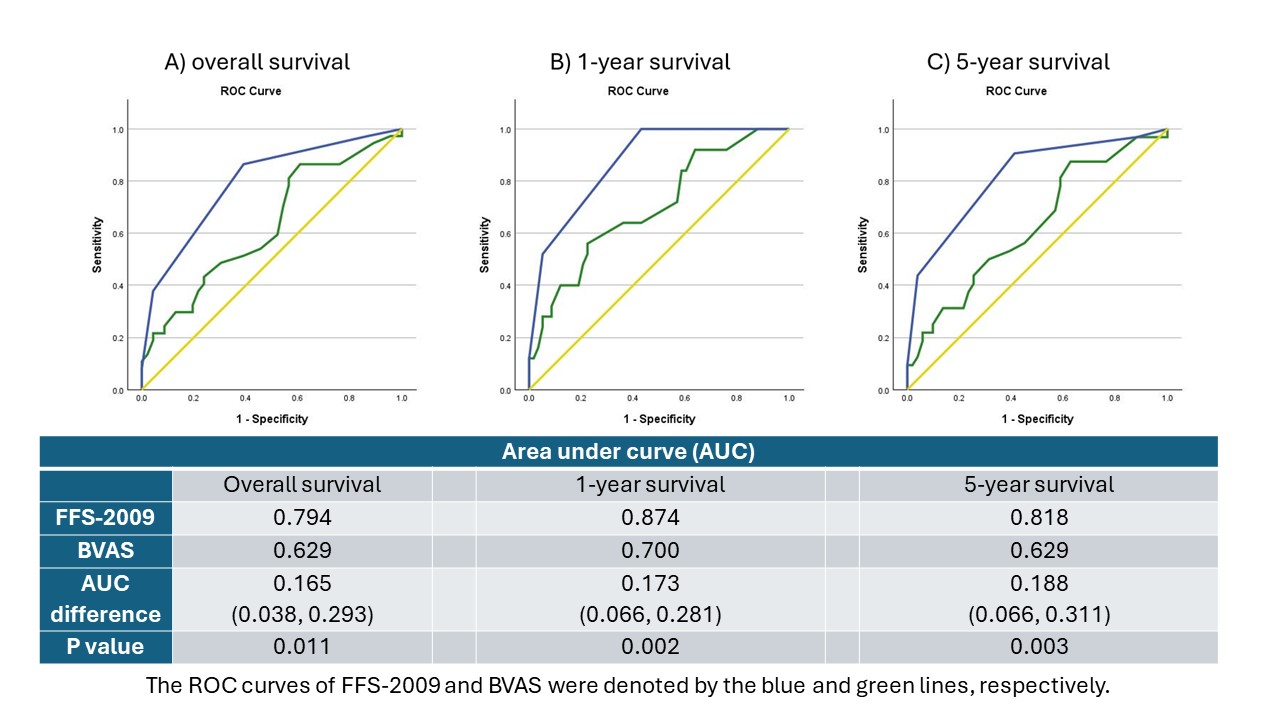
Results: 83 AAV patients were included with a median age of 70.5 years at diagnosis and 50.6% were male. The median follow-up duration was 23 months (IQR 3, 49). Baseline characteristics and clinical manifestations were shown in Table 1. MPA (69.9%) was the most common AAV clinical subtype, followed by EGPA (18.1%) and GPA (12.0%). MPA patients were significantly older at diagnosis, with frequent renal involvement (91.6%). Majority of MPA (98.3%) and EGPA (66.7%) cases were MPO-ANCA positive. All GPA cases were PR3-ANCA positive. Pulmonary-renal syndrome occurred in 12.0% of all cases. The median peak serum creatinine was 229 µmol/L (IQR 102, 553). Twenty-four patients (28.9%) had eGFR ≤ 10 mL/min/1.73m2 at initial diagnosis. The median FFS and BVAS were 2 and 20, respectively. The overall mortality was 45.6% across the study period. The leading causes of overall mortality were infection (70.3%) and active vasculitis (62.2%). Multivariate Cox regression identified age at diagnosis (HR 1.043, P = 0.027), stabilised peak serum creatinine (HR 1.002, P = 0.001), haemoglobin level (HR 0.754, P = 0.006), cardiac involvement (HR 3.862, P = 0.008), and use of non-glucocorticoid maintenance therapy (HR 0.261, P = 0.002) being independent predictors of overall mortality (Table 2). Both FFS and BVAS were significant predictors of mortality. The AUC of ROC curves suggested FFS was a good prediction tool for early mortality in 1 year, with an AUC value of 0.874 (Figure 1).
Conclusion: Our results echoes previous studies suggesting MPO-ANCA positive MPA is the most frequent AAV clinical subtype in Asian and Chinese. Over 60% of our cases fell into the worst FFS category group (FFS-2009 ≥ 2). Despite the advances in treatment, AAV still carried significant morbidities with high mortality. Baseline clinical features including age at diagnosis, stabilised peak serum creatinine, haemoglobin level, cardiac involvement, and use of non-glucocorticoid maintenance therapy were predictors of overall mortality. FFS at diagnosis appeared to be an easier and better tool in clinical practice to identify high risk cases.
To cite this abstract in AMA style:
Yeung K, Young K. Clinical Characteristics, Predictors for Mortality and Comparison of the Birmingham Vasculitis Activity Score and the Five-Factor Score on Survival in ANCA-associated Vasculitis in Hong Kong : A Multi-centre Retrospective Cohort Study [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/clinical-characteristics-predictors-for-mortality-and-comparison-of-the-birmingham-vasculitis-activity-score-and-the-five-factor-score-on-survival-in-anca-associated-vasculitis-in-hong-kong-a-multi/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-characteristics-predictors-for-mortality-and-comparison-of-the-birmingham-vasculitis-activity-score-and-the-five-factor-score-on-survival-in-anca-associated-vasculitis-in-hong-kong-a-multi/