Session Information
Session Type: Abstract Submissions (ACR)
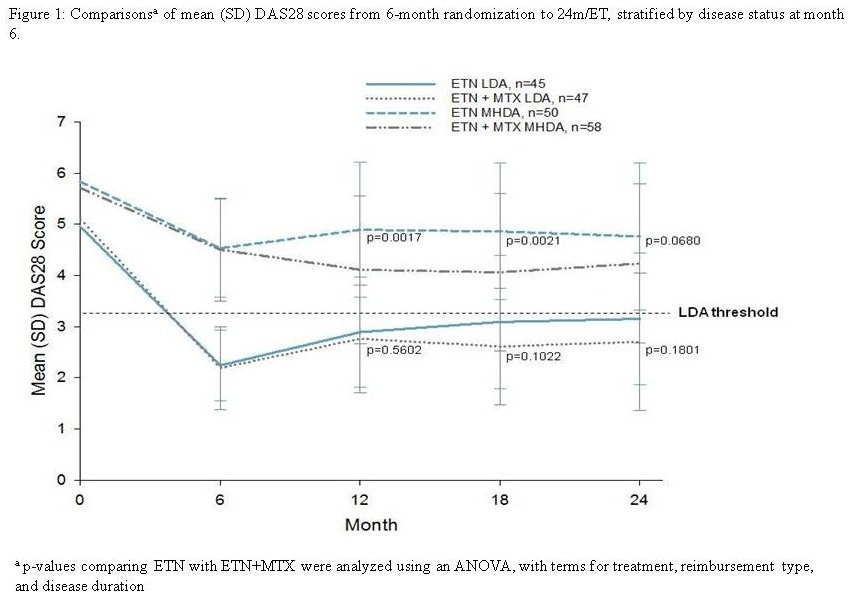
Background/Purpose: Data from the CAMEO study demonstrated that patients with rheumatoid arthritis (RA) who achieved low disease activity (LDA) after 6 months of combination therapy of etanercept (ETN) and methotrexate (MTX) had similar clinical outcomes at 12 months whether they continued ETN+MTX or stopped MTX at 6 months. Yet response was reduced when MTX was withdrawn in patients with moderate or high disease activity (MHDA). Clinical and radiographic data for up to 24 months from the CAMEO study are presented.
Methods: TNF-inhibitor naïve patients with active RA (defined as ≥3 swollen joints and a Disease Activity Score [DAS28] ≥3.2) despite treatment with MTX (≥15 mg/week, or 10 mg/week if intolerant) for >12 weeks were treated with ETN (50 mg/week SC) and MTX for 6 months. Patients were then randomized (1:1) to switch to ETN monotherapy or to continue ETN+MTX for an additional 18 months. DAS28 was assessed at baseline and at 6, 12, 18, and 24 months/early termination (24m/ET), and X-rays of the hands and feet were taken at baseline and at 12 and (24m/ET).
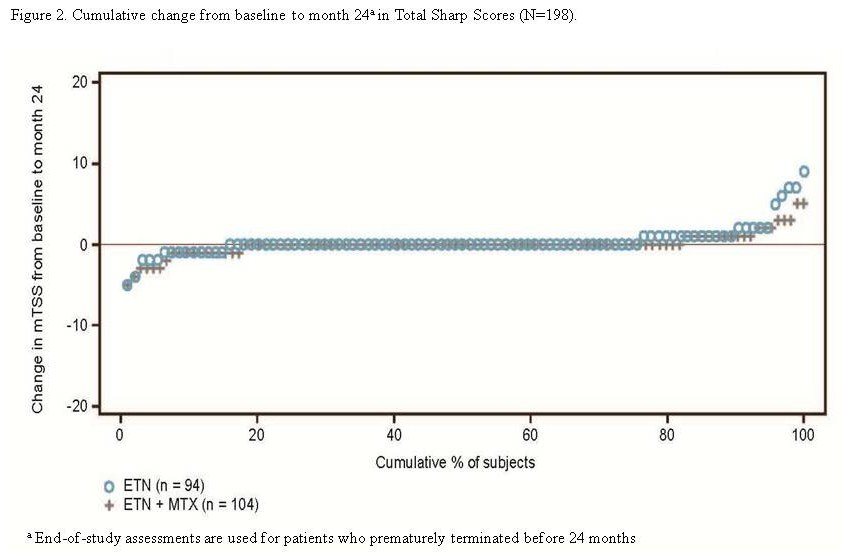
Results: A total of 258 patients enrolled, and 205 were randomized to either begin ETN monotherapy (n=98) or to continue ETN+MTX treatment (n=107). Seventy-six percent were females with a mean age of 54.7±12.5 years, disease duration of 8.9±8.4 years, and baseline DAS28 score of 5.4±1.1. Overall, patients who reached LDA at month 6 maintained LDA at (24m/ET) whether they were treated with ETN or ETN+MTX; those with MHDA treated with ETN monotherapy had worsening of disease activity, while those treated with ETN+MTX had a sustained response (Figure 1). Radiographic progression between patients treated with ETN or ETN+MTX was similar at 24 months (Figure 2). The proportion of patients with LDA showing no radiographic progression was similar between the ETN and ETN+MTX at both 12 (88% vs. 85%) and (24m/ET) (86% vs. 87%). However, fewer patients with MHDA receiving ETN monotherapy had no radiographic progression compared with ETN+MTX at 12 (68% vs. 81%) and (24m/ET) (64% vs. 76%).
Conclusion: These data clarify the role of long term combination of ETN+MTX in maintaining optimal disease control. For patients who achieve LDA by 6 months, ETN monotherapy provides an effective clinical and radiological alternative to combination therapy for up to 24 months. However, patients with MHDA may need to continue combination therapy, as clinical response may be reduced when MTX is withdrawn.
Disclosure:
B. Haraoui,
Amgen,
5,
Abbott Laboratories,
5,
Bristol-Myers Squibb,
5,
Merck Pharmaceuticals,
5,
Pfizer Inc,
5,
Roche Pharmaceuticals,
5,
UCB,
5;
J. C. Thorne,
Amgen,
5,
Pfizer Inc,
5,
Abbott Laboratories,
5,
Bristol-Myers Squibb,
5,
Centocor, Inc.,
5,
Merck Pharmaceuticals,
5,
Roche Pharmaceuticals,
5,
UCB,
5;
E. C. Keystone,
Abbott Laboratories,
5,
Amgen,
5,
AstraZeneca,
5,
Bristol-Myers Squibb,
5,
Centocor, Inc.,
5,
Hoffmann-La Roche, Inc.,
5,
Genzyme Corporation,
5,
Merck Pharmaceuticals,
5,
Novartis Pharmaceutical Corporation,
5,
Pfizer Inc,
5,
UCB,
5,
Genentech and Biogen IDEC Inc.,
5,
Nycomed,
5;
M. Poulin-Costello,
Amgen,
3;
E. Trottier,
Amgen,
3;
A. Vieira,
Amgen,
3;
J. E. Pope,
Amgen,
2,
Pfizer Inc,
2.
« Back to 2013 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-and-radiographic-outcomes-with-etanercept-and-etanercept-and-methotrexate-in-patients-with-rheumatoid-arthritis-two-year-results-from-the-canadian-methotrexate-and-etanercept-outcome-study/