Session Information
Session Type: Abstract Session
Session Time: 8:00AM-9:00AM
Background/Purpose: Studies report ~83% of SLE patients discontinue hydroxychloroquine (HCQ) and many report suboptimal shared decision-making with their healthcare team. Moreover, patients report knowledge gaps on role of HCQ in improving survival in SLE, and inflated concerns about rare eye toxicity. In complex diseases, involving patients as partners to make therapy decisions can improve adherence and outcomes. Further, AHRQ calls for interventions meeting low health literacy standards. The objective was to describe the development and piloting of a decision aid (HCQ-SAFE) to facilitate shared decision making about HCQ’s safety and efficacy.
Methods: Based on prior decision aid development, HCQ-SAFE was developed via a collaborative process involving patients, clinicians, implementation scientists, and health literacy experts. Prototyping was informed by AHRQ low literacy principles and key themes about HCQ use from six patient & clinician focus groups. Experts (n=4) reviewed the first prototype and guided an iterative process to revise subsequent prototypes which were then reviewed and endorsed by patients (n=11) and clinicians (n=9). The final decision aid was implemented in four clinics during 40 visits to examine usability and feasibility. Usability was measured by patient-reported understanding of HCQ’s role in SLE after using HCQ-SAFE, and resolution of any decisional conflicts. We used a Likert scale to measure users’ likelihood to recommend HCQ-SAFE (NPS= net promoter score). We included “Extremely or very likely” as promoters and “extremely or very unlikely” as detractors and calculated NPS = %promoters – %detractors. Next, feasibility was determined by measuring percentage of visits using HCQ-SAFE, percent completed by a non-MD, and time spent to review HCQ-SAFE.
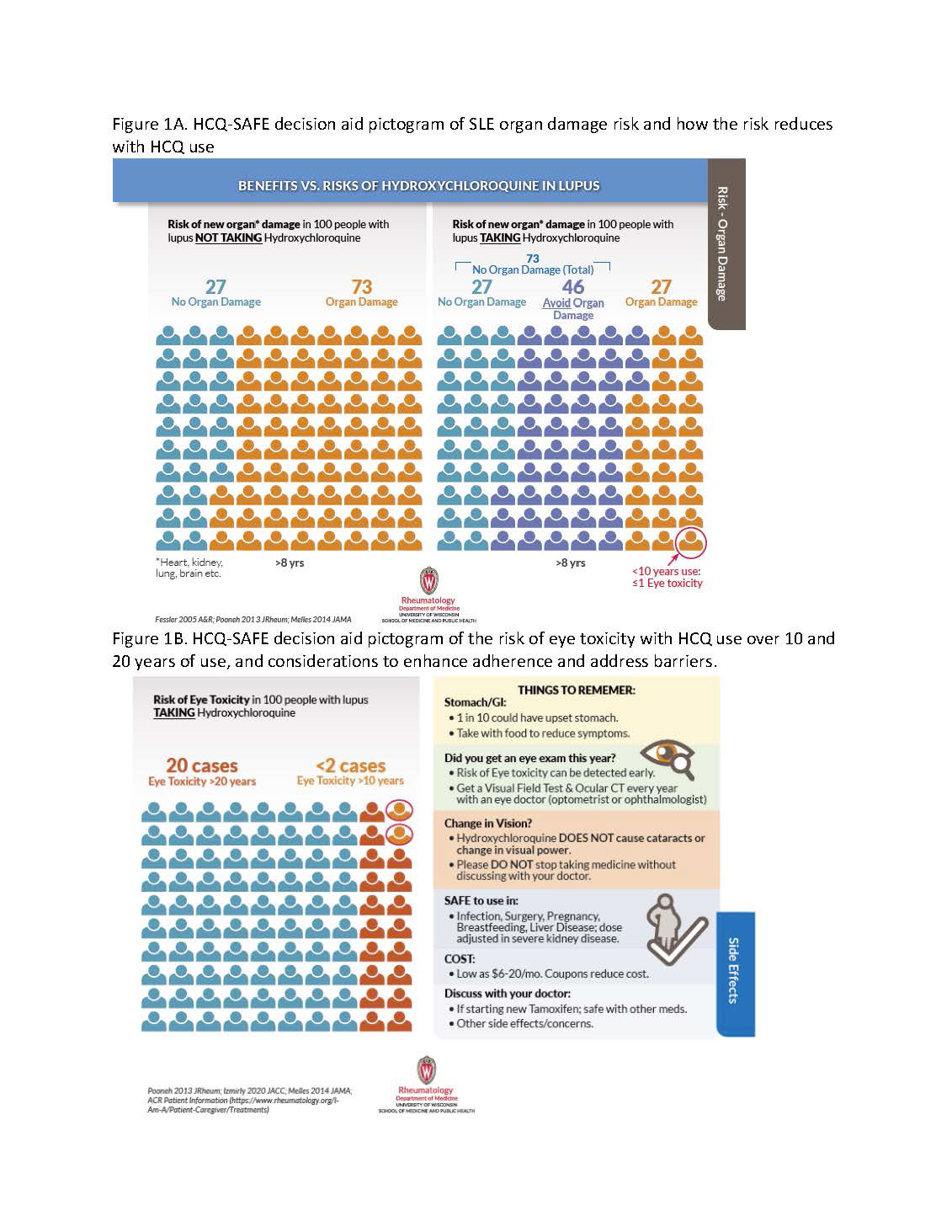
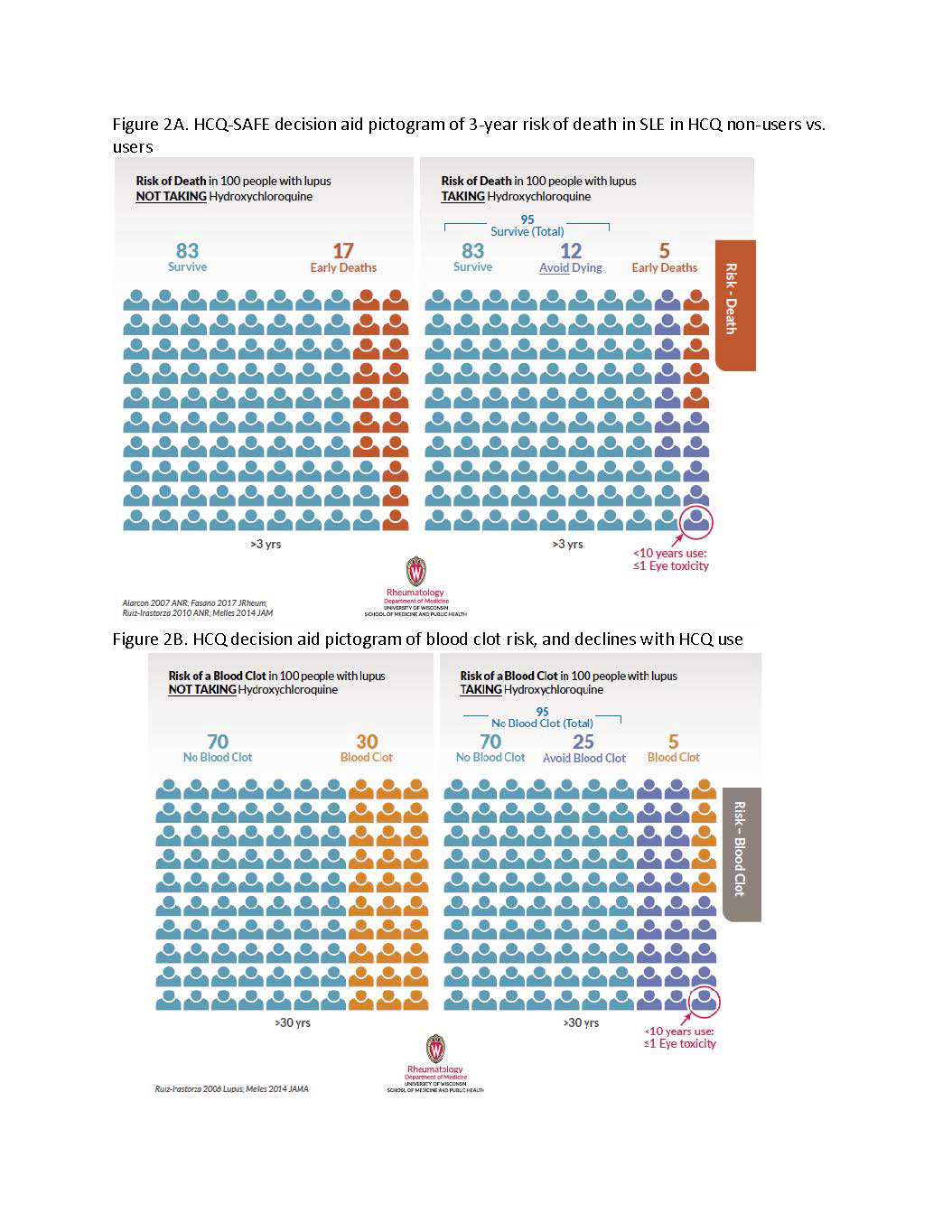
Results: The final HCQ-SAFE evidence-based shared decision-making laminated tool has data organized using pictograms and plain language across four risks of interest: a) organ damage, b) premature death, c) blood clots, & d) eye toxicity in HCQ users vs. non-users.
During visits a patient and clinician first review pictograms of organ damage risk in SLE, then see how risks decrease with HCQ (Fig 1A). Next, declines in risks of early death and blood clots in HCQ users (Fig 2A-B) vs. low risk of eye toxicity are reviewed (Fig 1B & circles in Fig 1A-2).
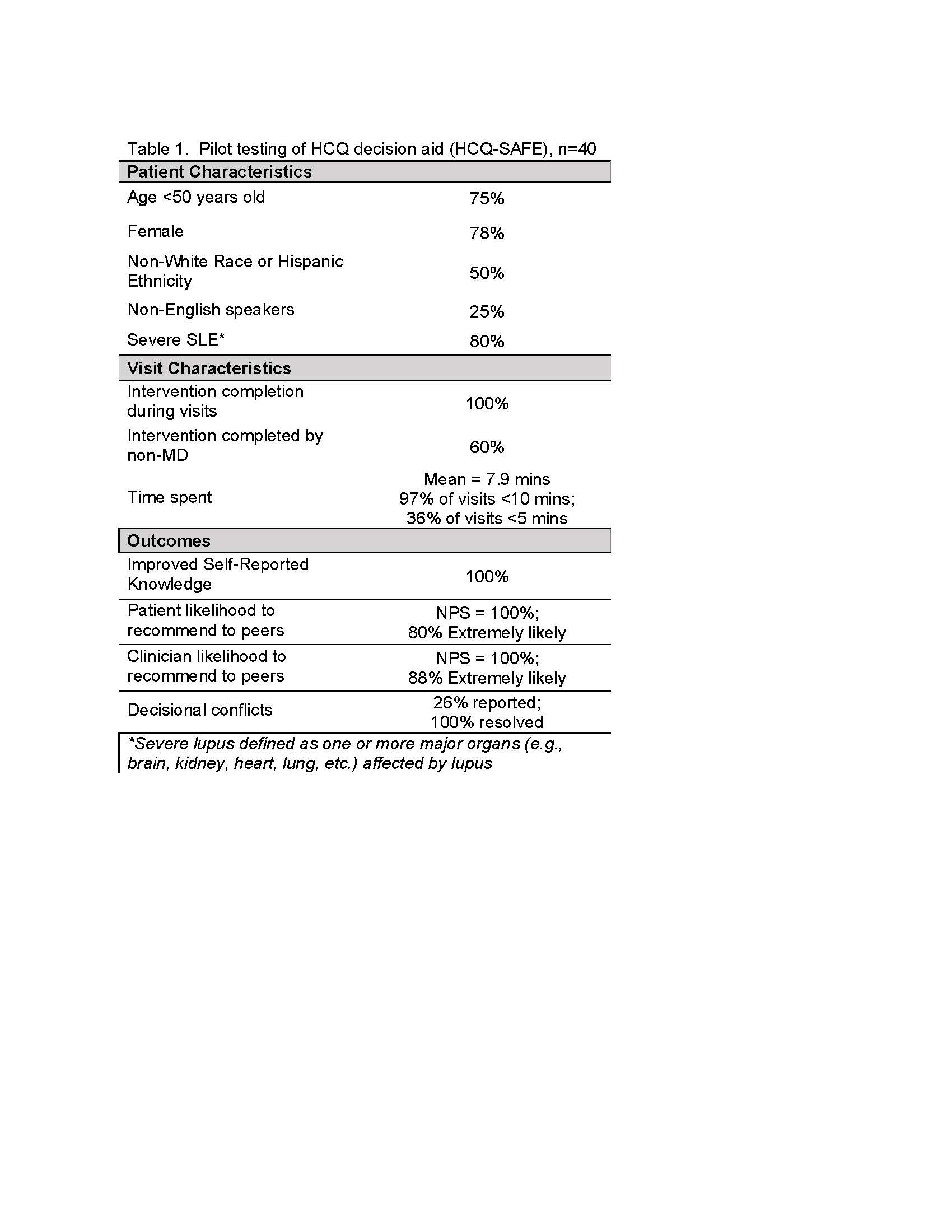
We used HCQ-SAFE during 40 patient visits, including 25% non-English speaking patients. All patients reported improved knowledge about damage-free survival benefits of HCQ in SLE (Table 1). Moreover, HCQ-SAFE increased patients requesting an eye referral for HCQ screening by 25%. Decisional conflicts were noted in 26% of visits that all resolved using HCQ-SAFE. HCQ-SAFE garnered high clinician & patient support and high likelihood to recommend (NPS = 100%; avg Likert score = 8.5). Finally, 97% of clinicians reported spending < 10 mins. to review HCQ-SAFE; 60% of discussions were led by a non-MD.
Conclusion: We created HCQ-SAFE, an evidence-based, feasible shared decision-making tool with patients and experts. HCQ-SAFE aims to enhance communication to improve knowledge, clarify misbeliefs, and engage patients in treatment decisions, including those with limited health literacy and proficiency in English.
To cite this abstract in AMA style:
Garg S, Ferguson S, Chewning B, Gomez S, Keevil J, Bartels C. Clarifying Misbeliefs About Hydroxychloroquine (HCQ): Developing an Evidence-Based HCQ Benefits vs. Risk Decision Aid (HCQ-SAFE) Per Low Health Literacy Standards [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/clarifying-misbeliefs-about-hydroxychloroquine-hcq-developing-an-evidence-based-hcq-benefits-vs-risk-decision-aid-hcq-safe-per-low-health-literacy-standards/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clarifying-misbeliefs-about-hydroxychloroquine-hcq-developing-an-evidence-based-hcq-benefits-vs-risk-decision-aid-hcq-safe-per-low-health-literacy-standards/