Session Information
Date: Sunday, November 12, 2023
Title: (0252–0282) Miscellaneous Rheumatic & Inflammatory Diseases Poster I
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
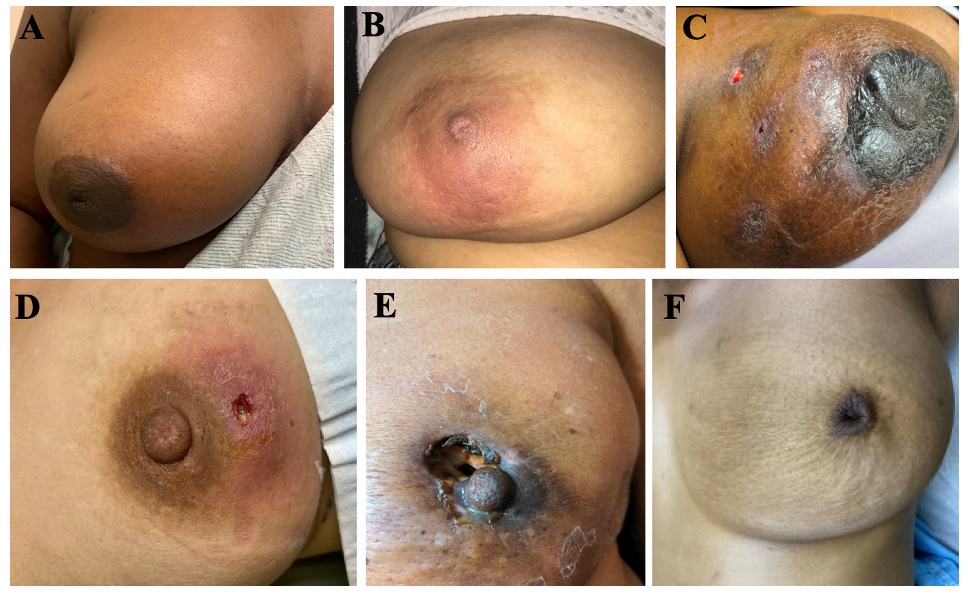
Background/Purpose: Granulomatous mastitis (GM) is a rare, chronic, inflammatory breast condition characterized by granulomatous inflammation affecting mainly minority women of childbearing age. Patients present with breast mass and pain that can progress to abscess, fistula, sinus, or ulcer (Figure 1). Pathogenesis of GM is unknown. Hypotheses include autoimmune, inflammatory, infectious, or benign causes. Management includes antibiotics, anti-inflammatory drugs, corticosteroids, disease-modifying anti-rheumatic drugs, biologics, and surgery.
Methods: We performed an IRB-approved retrospective analysis of patients with GM at Montefiore between 1/1/2014-1/1/2023. Inclusion criteria were age greater than 18, diagnosis of GM (clinically diagnosed or biopsy proven). Exclusion criteria were age younger than 18, concurrent alternate breast pathology. We identified 119 patients with GM. No patients fit exclusion criteria.
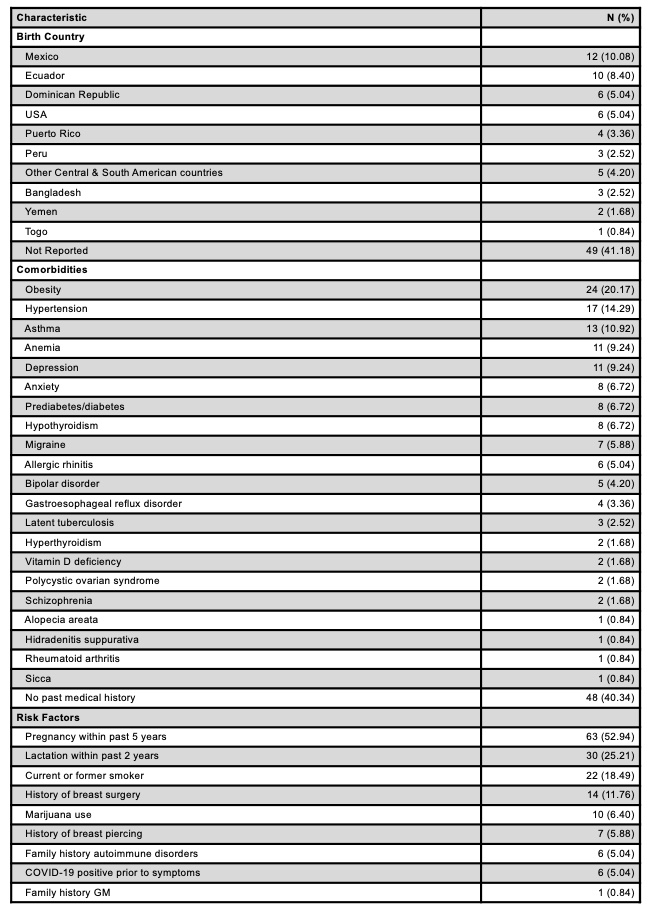
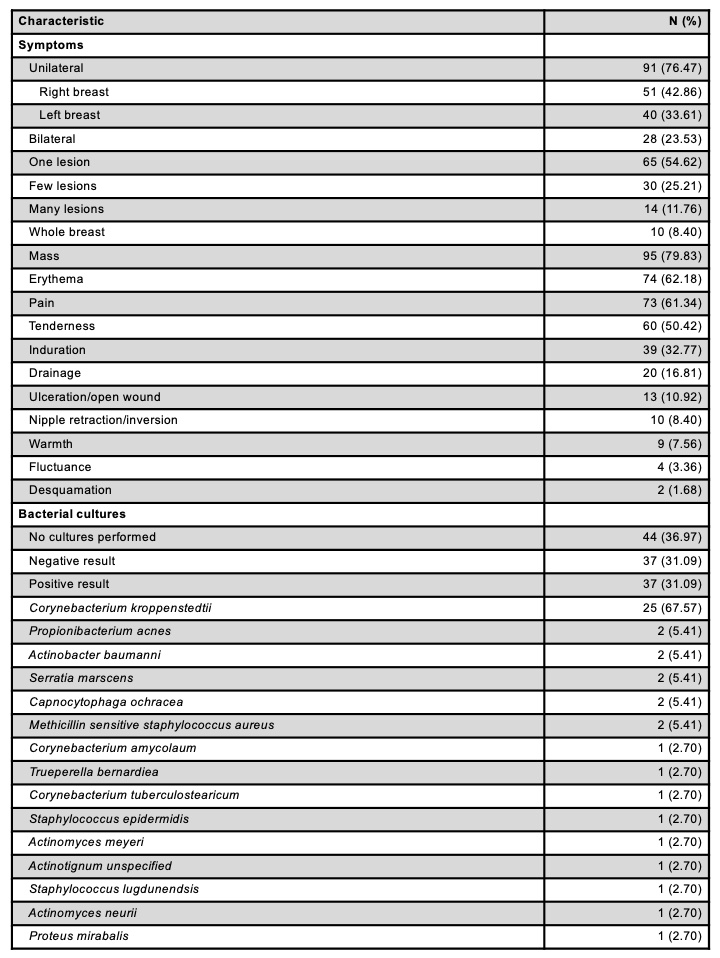
Results: 119 patients (118 female, 1 male) with GM were identified. Mean age at diagnosis was 36.29 years (range 20-83). Most patients were minorities (Hispanic/Latino 48.74%, African American 21.01%, Other/Unknown 19.33%, Caucasian 5.88%, Asian 4.20%) and hailed from a broad range of countries (Table 1). Most common comorbidity was obesity (20.17%) and major risk factors included pregnancy within 5 years (52.94%), lactation within 2 years (25.21%), and former/current smoker (18.49%) (Table 1). Most patients experienced unilateral symptoms (76.47%) of breast mass (79.83%), erythema (62.18%), pain (61.345%), and tenderness (50.42%) (Table 2). Mean symptom duration prior to presentation was 53.27 days (range 1-365) and symptom duration prior to diagnosis was 188.96 days (range 3-2555). Of 37 patients with positive bacterial cultures, 67.57 % had Corynebacterium kroppenstedtii (Table 2). 84.87% were biopsied and patients not biopsied were diagnosed with a combination of clinical presentation, imaging, and treatment response. Ultrasound, mammogram, and MRI were performed in 109, 82, and 8 patients, respectively. Most common BIRADS score was 4 for ultrasound (33.94%) and for mammogram (31.71%). Antibiotics were prescribed to 84.03% of patients, most commonly doxycycline (49.00%), bactrim (41.00%), and clindamycin (36.00%). Steroid immunotherapy and methotrexate were prescribed to 69.75% and 14.29% of patients, respectively. Surgical interventions included incision and drainage (43.70%) and excision (12.61%). 3 months, 1 year, and 2 years after symptom onset, 79.81%, 40.38%, and 18.27% of patients had persistent symptoms, respectively. Recurrence occurred in 6 patients.
Conclusion: This is the largest retrospective case series of GM in the United States to date. We stratified comorbidities and risk factors in patients with GM and identified several bacteria previously not reported including Capnocytophaga ochracea, Serratia marscens, Actinomyces meyeri, Actinomyces neurii, Trueperella bernardiea, Actinotignum unspecified, and Proteus mirabalis. Combining clinical anecdotal evidence with this comprehensive review, we advise physicians caring for young, female, minority patients with breast pain, mass, erythema, or drainage to be mindful for developing GM.
To cite this abstract in AMA style:
Pattison L, Ayesha B, Kumthekar A, McEvoy M, McLellan B, Gendlina I. Characterizing Granulomatous Mastitis: A Retrospective, Single-Institutional Case Series of a Racially and Ethnically Diverse Cohort [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/characterizing-granulomatous-mastitis-a-retrospective-single-institutional-case-series-of-a-racially-and-ethnically-diverse-cohort/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/characterizing-granulomatous-mastitis-a-retrospective-single-institutional-case-series-of-a-racially-and-ethnically-diverse-cohort/