Session Information
Session Type: Abstract Session
Session Time: 2:00PM-3:30PM
Background/Purpose: Telehealth in rheumatology rapidly expanded in the wake of the COVID-19 pandemic, however it remains unknown how provider perceptions of telehealth changed as the pandemic evolved and providers gained additional experience with telehealth. In this project, we describe rheumatology providers’ perceptions of telehealth appropriateness from 2021 – 2022, along with the clinical and demographic factors that align with telehealth appropriateness.
Methods: Providers at a single academic rheumatology practice in the U.S. documented their perception of telehealth appropriateness by recording the Encounter Appropriateness Score for You (EASY) in their progress notes immediately following each in-person or telehealth encounter. The EASY score asks providers, “Which of the following encounter types would have been most appropriate for TODAY’S visit? (Irrespective of the pandemic).” Response options include: (1) Either in-person or telehealth acceptable; (2) In-person preferred; (3) Telehealth preferred. For this analysis, EASY scores 1 and 3 were consolidated into a single variable, “telehealth acceptable.” We analyzed changes in EASY scores and encounter modality from 1/1/2021 – 10/30/2022. In addition, we analyzed the distribution of EASY scores according to patient demographic and clinical variables. This analysis was limited to return encounters.
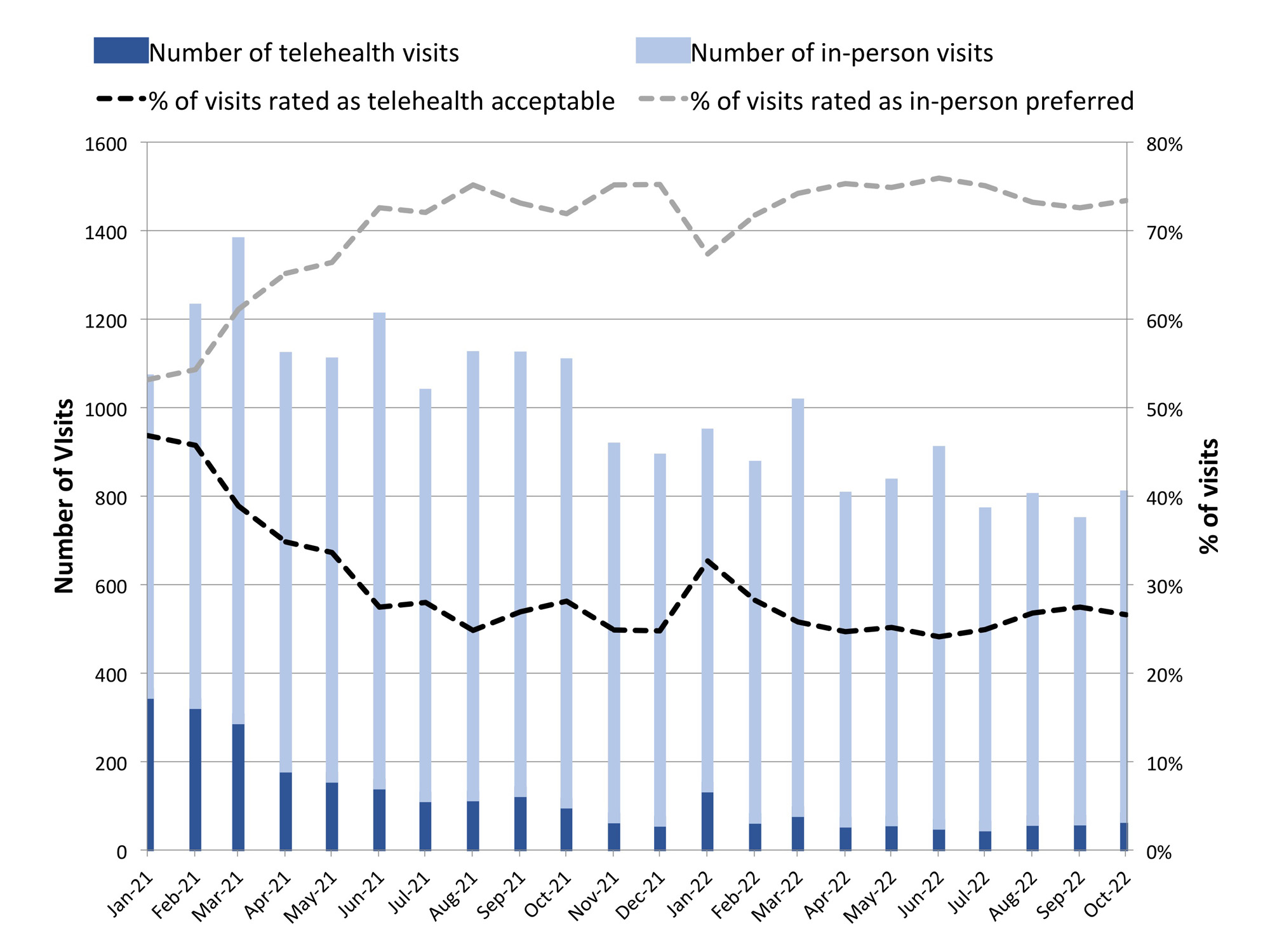
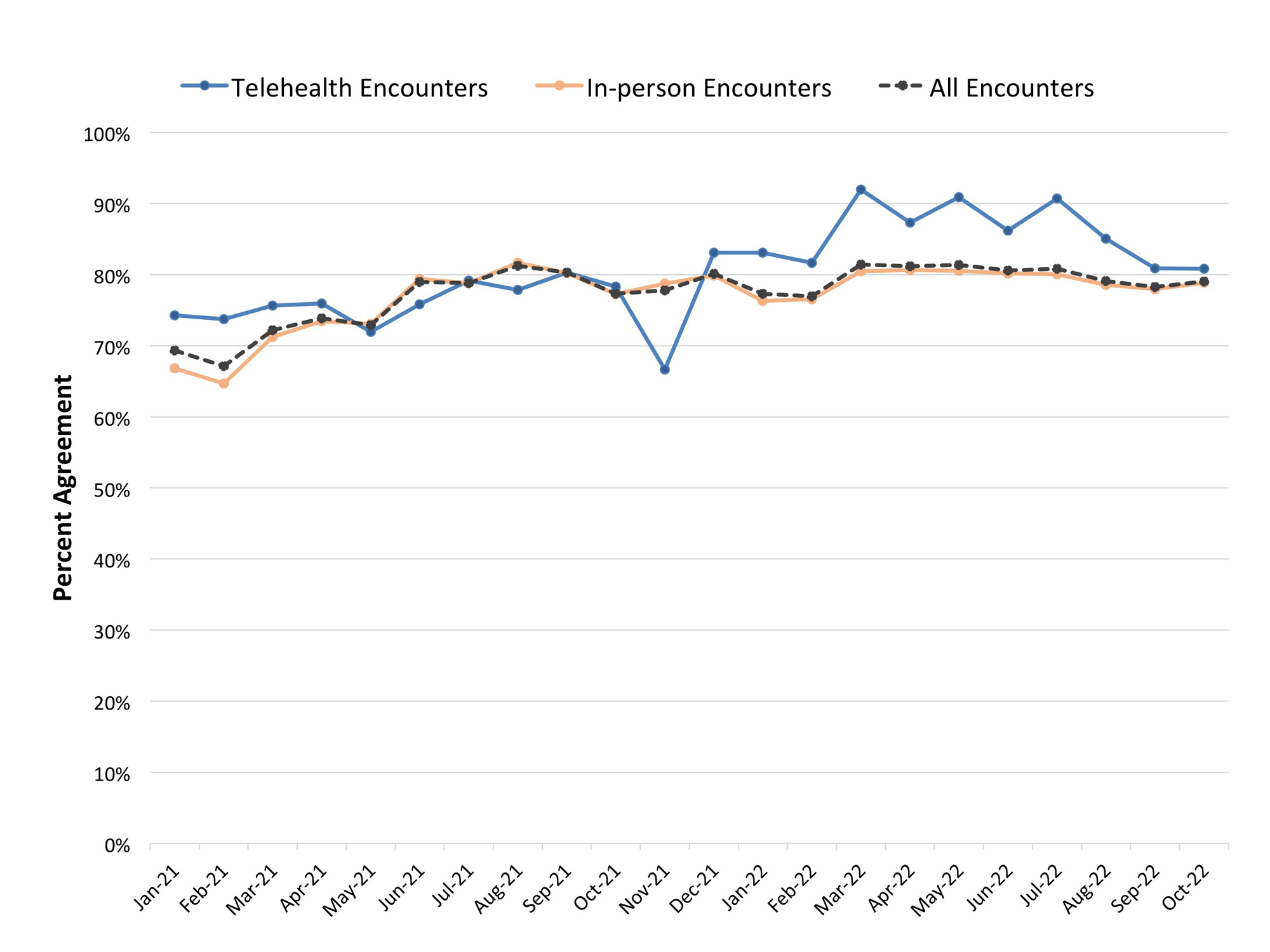
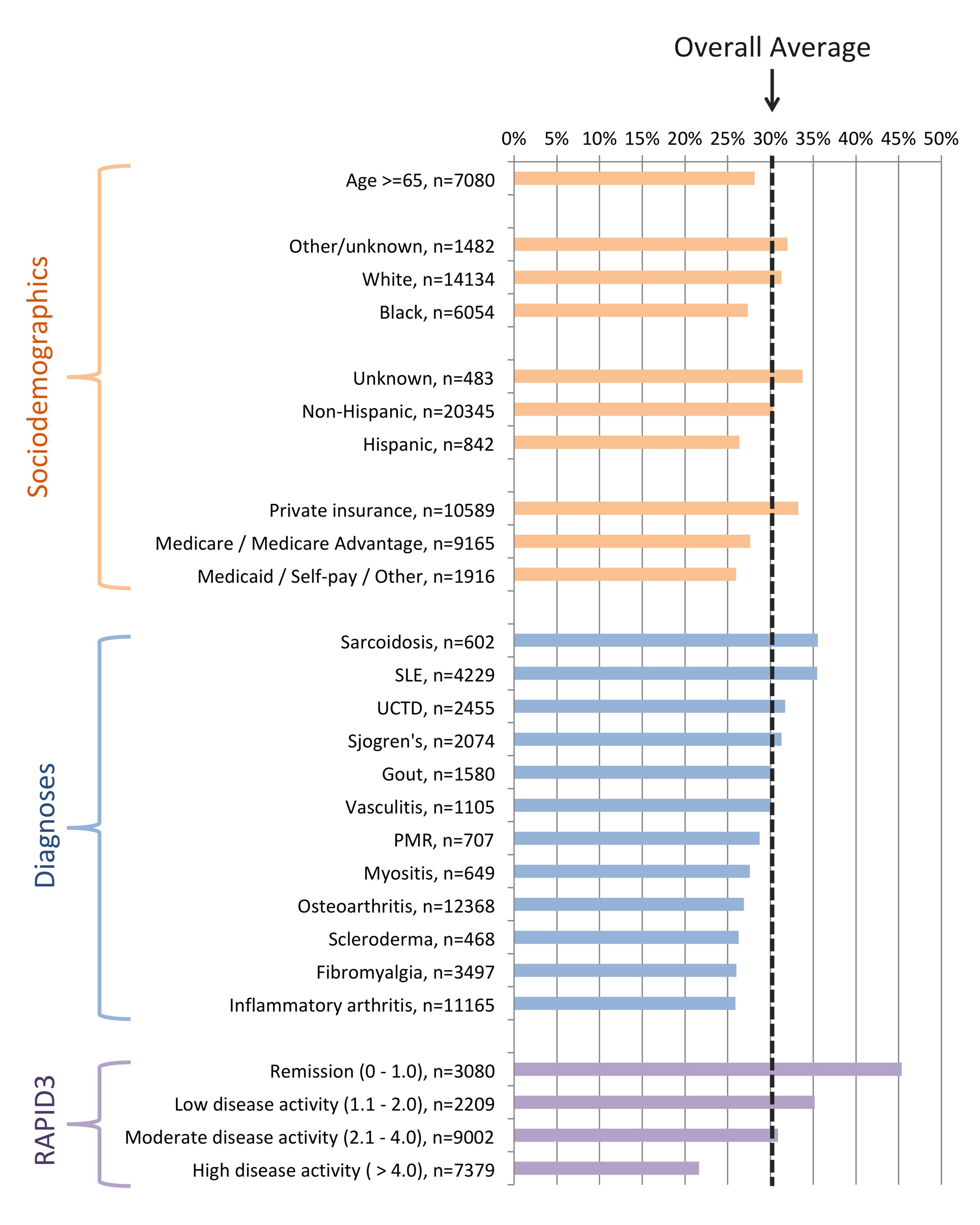
Results: Over the study period, 27 providers documented EASY scores for 21,670 return encounters. Of these, 6,551 (30.2%) were rated as telehealth acceptable and 15,119 (69.8%) in-person preferred. The proportion of EASY scores rated as telehealth acceptable declined over time, from approximately 47% in January 2021 to 25% from August 2021 – October 2022 (Figure 1). The proportion of visits that occurred by telehealth also declined from 33% in January 2021 to approximately 15% in 2022. The proportion of EASY scores matching the actual encounter type (indicating the appropriate type of visit actually occurred) increased for all encounters from 69% in January 2021 to approximately 80% throughout 2022 (Figure 2). Among the 27 providers, there was substantial variability in the proportion of visits each provider rated as telehealth acceptable (median 35%, IQR 12-43%, full range 3-72%). Patient characteristics, including demographics, diagnoses, and patient-reported symptom severity (RAPID3), were related to telehealth appropriateness (Figure 3), with the most telehealth acceptance among patients with RAPID3 scores indicating remission (45%) and the least acceptance with high disease activity (22%).
Conclusion: Providers became progressively less likely to consider a visit appropriate for telehealth over the first half of 2021, but then stabilized estimating approximately 25% of all return visits telehealth-appropriate. Frequency of telehealth visits followed a similar pattern, though generally telehealth visits accounted for fewer than 25% of visits in 2022, suggesting that telehealth is under-utilized. For example, providers report telehealth as appropriate in over 35% of encounters when the patient reports low symptom severity, suggesting that this sub-population of patients could be a good target for increased telehealth use.
To cite this abstract in AMA style:
Leverenz D, Solomon M, Henao R, Smith I, Howe C, Economou-Zavlanos N, Adagarla B, Coles T, Overton A, Doss J, Clowse M. Changes in Rheumatology Providers’ Perceptions of Telehealth Appropriateness from 2021 to 2022 [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/changes-in-rheumatology-providers-perceptions-of-telehealth-appropriateness-from-2021-to-2022/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/changes-in-rheumatology-providers-perceptions-of-telehealth-appropriateness-from-2021-to-2022/