Session Information
Date: Monday, November 9, 2020
Title: Pediatric Rheumatology – Clinical II: Outcomes & Care Delivery (1983–1987)
Session Type: Abstract Session
Session Time: 10:00AM-10:50AM
Background/Purpose: The relative roles of disease activity and disability as determinants of health-related quality of life (HRQoL) in children with JIA have been controversial; sometimes their statistical significance disappears when pain is added to multivariate models. We explored whether structural equation modelling (SEM) may help clarify the causal pathways leading to decreased HRQoL in children with JIA. SEM estimates direct and indirect effects of candidate determinants along a causal pathway and uses multiple indicators to study determinants that are imperfectly quantified, such as disease activity and treatment intensity.
Methods: We used data from the Research in Arthritis in Canadian Children emphasizing Outcomes (ReACCh-Out) cohort. Based on published literature and clinical plausibility we proposed a priori models with explicit root causes (disease activity, treatment intensity) and mediators (pain, disease symptoms, function) leading to HRQoL measured with the Quality of my Life scale (QoML, 0=worst, 10=best) and the Juvenile Arthritis Quality of Life Questionnaire (JAQQ, 1=best, 7=worst), at five stages of disease: 1) diagnosis (within 28 days), 2) 3-9 months after diagnosis, 3) flare, 4) remission on medications, and 5) remission off medications. SEM was applied to the data and a posteriori models were selected based on fit statistics, parameter estimates, and plausibility. Here we focus on the models for QoML at diagnosis.
Results: We included 563 children with assessments of HRQoL within 28 days of diagnosis (Table 1). The a priori model is shown in Figure 1, where the direction and magnitude of hypothesized effects are depicted by the number of + or – signs. Figure 2 shows the a posteriori model with the best fit, where path coefficients estimated by SEM (numbers in Figure 2) quantify the observed direction and magnitude of effect. Comparison of the two figures shows that most hypothesized effects were supported, with a few modifications: 1) Drug categories and Discomforts and concerns were eliminated due to overlap or for lack of measures; 2) The paths from disease activity first to pain, functional deficit (CHAQ DI) and disease symptoms are supported; 3) Participation restrictions is a subsequent common intermediary, as proposed; 4) A direct path from treatment to QoML is the only one supported, whereas the path through side effects is not significant; 5) Pain, participation restrictions and effects of treatment not mediated by side effects are then the immediate determinants of QoML. In results not shown, models for 3-9 months after diagnosis and flare were similar to that at diagnosis and largely supported the hypothesized relationships (path coefficients 0.1 to 1.0 in the expected direction). Models for JAQQ provided greater specificity as to the domains of HRQoL affected. Models for remission stages were unsatisfactory.
Conclusion: Using SEM, we found support for disease activity and treatment intensity as root determinants of decreased HRQoL in children with JIA. Disease activity acts mainly via pain, functional impairments and participation restrictions. Treatment main effects at diagnosis were not mediated by side effects.
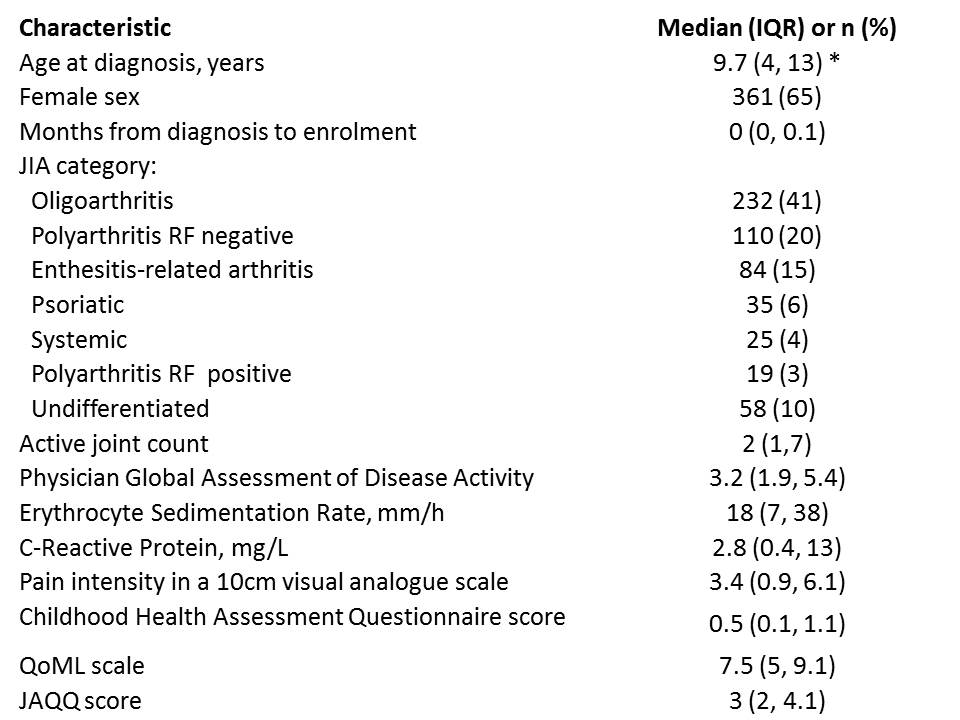 Table 1: Baseline characteristics of 563 children with HRQoL assessments within 28 days of diagnosis in the ReACCh-Out cohort
Table 1: Baseline characteristics of 563 children with HRQoL assessments within 28 days of diagnosis in the ReACCh-Out cohort
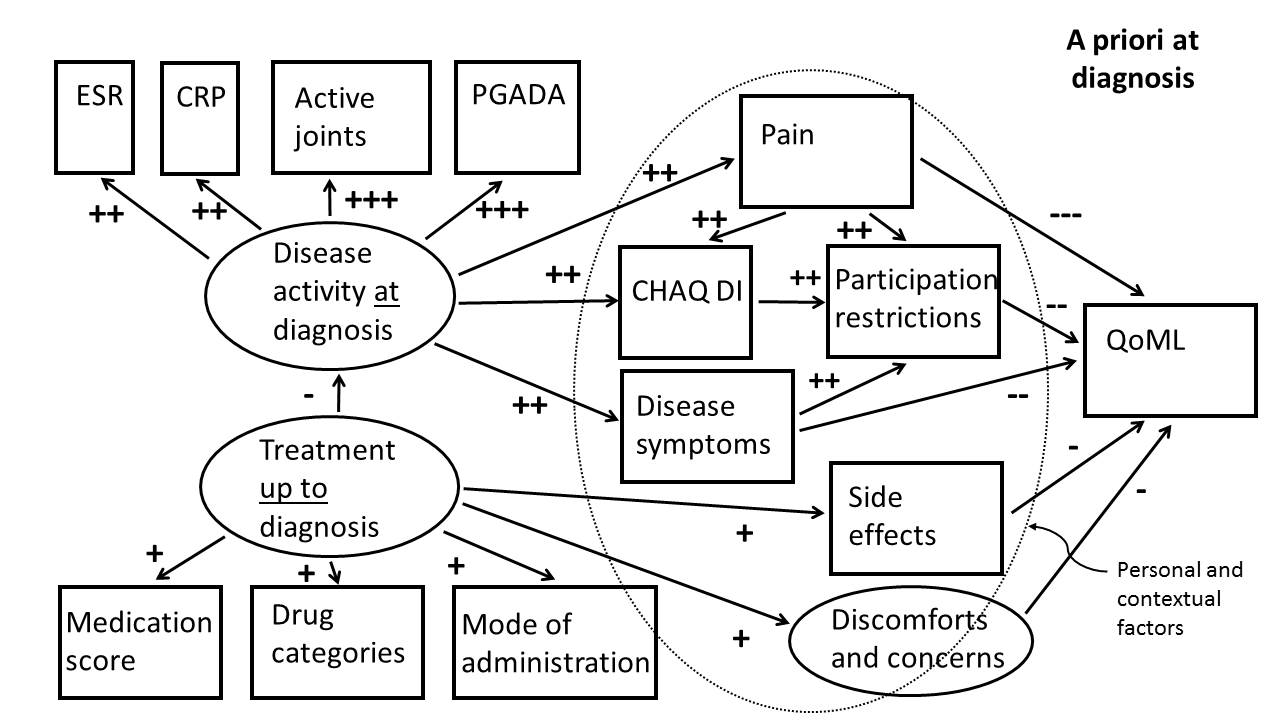 Figure 1: Hypothesized a priori model of the causal pathways leading to HRQoL at diagnosis as measured by QoML. ESR, CRP, active joint count and physician global assessment of disease activity (PGADA) are proposed as measures of disease activity; and medication score, drug categories and mode of administration as measures of treatment intensity. Disease activity and treatment intensity have proposed effects on mediators, such as pain, other symptoms and function which in turn impact HRQoL. Personal and contextual factors were not analysed.
Figure 1: Hypothesized a priori model of the causal pathways leading to HRQoL at diagnosis as measured by QoML. ESR, CRP, active joint count and physician global assessment of disease activity (PGADA) are proposed as measures of disease activity; and medication score, drug categories and mode of administration as measures of treatment intensity. Disease activity and treatment intensity have proposed effects on mediators, such as pain, other symptoms and function which in turn impact HRQoL. Personal and contextual factors were not analysed.

To cite this abstract in AMA style:
Oen K, Tian J, Loughin T, Berard R, Chan M, Duffy C, Feldman B, Huber A, Levy D, Rumsey D, Shiff N, Tse S, Tucker L, Watanabe-Duffy K, Guzman J. Causal Pathways to Health-Related Quality of Life in Children with Juvenile Idiopathic Arthritis: Results from the ReACCh-Out Cohort [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/causal-pathways-to-health-related-quality-of-life-in-children-with-juvenile-idiopathic-arthritis-results-from-the-reacch-out-cohort/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/causal-pathways-to-health-related-quality-of-life-in-children-with-juvenile-idiopathic-arthritis-results-from-the-reacch-out-cohort/