Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Carpal tunnel syndrome (CTS) is a common complication of rheumatoid arthritis (RA). However, the occurrence of CTS before RA and the effect of RA serological status on CTS is not well understood. We aimed to assess the occurrence of CTS before and after RA incidence and by serological status compared to individuals without RA.
Methods: This retrospective population based cohort study included residents of a geographically defined area meeting the 1987 ACR classification criteria for RA between 1980 and 2019. Patients with RA were matched 1:1 with non-RA individuals by age, sex, and RA incidence year. All individuals were followed until death, migration, or 12/31/2023. At least two diagnosis codes no less than 30 days apart were used to identify CTS. Cumulative incidence of CTS adjusting for competing risk of death was assessed. Logistic regression and Cox proportional hazard models were used.
Results: We included 1335 patients with RA (mean age: 56.1 years, 69% females, 63% RF/CCP seropositivity), and 1331 individuals without RA. With a median of 32.5 and 32.9 years of prior medical history in the RA and non-RA individuals, respectively, the overall prevalence of CTS at any time prior to or at RA incidence was 179 (13%) in patients with RA compared to 85 (6%) in non-RA individuals (odds ratio (OR): 2.30; 95% CI: 1.75-3.03). The prevalence of CTS was increased 2 years or more prior to RA incidence/index (OR: 1.55; 95% CI: 1.14-2.10). Among the RA individuals, CTS prior to RA incidence was somewhat more common in RF/CCP negative (76; 15%) than positive (103; 12%) patients, but this association did not reach statistical significance (OR: 1.27; 95% CI: 0.92-1.76).
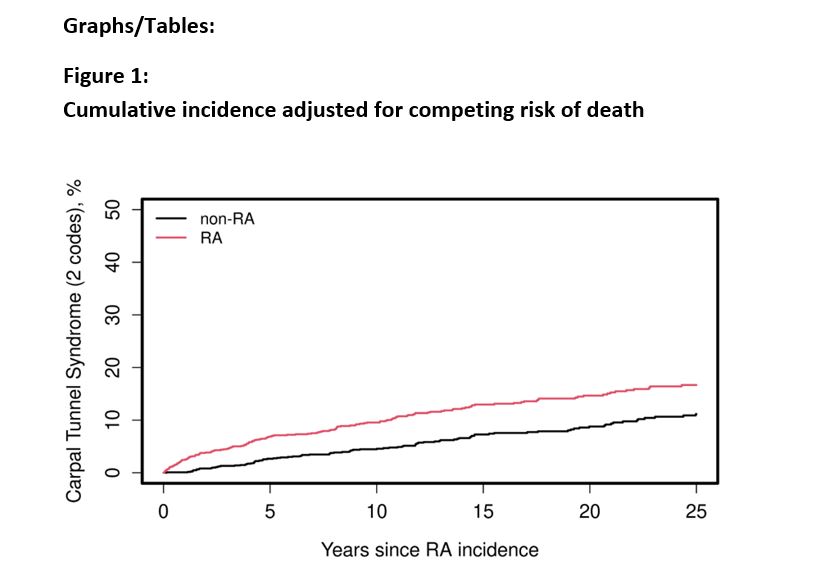
During median follow-up of 12.8 and 13.8 years in RA and non-RA, respectively, 154 patients with RA and 102 non-RA developed CTS. After adjusting for age and sex, individuals with RA were 82% more likely to develop CTS when compared to those without RA (age- and sex-adjusted hazard ratio: 1.82; 95% CI: 1.42-2.34) (Figure 1). When further adjusted for age, sex, smoking, and obesity, this association persisted (HR: 1.80, CI: 1.39-2.31).
We found a 37% increase in CTS incidence in patients with seronegative versus seropositive RA, although the difference did not reach statistical significance (age, sex smoking and obesity adjusted hazard ratio: 1.37, CI: 0.99-1.89).
Risk factors for development of CTS after RA incidence included increased BMI (HR: 1.03 per 1 kg/m2, CI: 1.01-1.06) and a lower erythrocyte sedimentation rate (ESR) at RA incidence (HR: 0.99 per 1 mm/hr, CI: 0.98-1.00).
Conclusion: Our study shows that CTS was 1.5-fold more common in individuals with RA (vs non-RA) two years or more prior to RA incidence/ index date, suggesting that it can be an early unrecognized feature of RA disease presentation. The incidence of CTS after RA incidence/ index date is significantly higher in patients with RA versus non-RA controls. Of note, patients with seronegative RA tend to have a higher prevalence of CTS prior to RA and a higher risk of developing CTS after RA onset (vs seropositive RA). These findings suggest the need for increased awareness of the risk of developing RA in patients with persistent CTS and consideration for early rheumatology referral in patients with a high degree of suspicion.
To cite this abstract in AMA style:
George R, Frechette N, Javed I, Kimbrough B, Achenbach S, Joerns E, Kronzer V, Davis J, Crowson C, Myasoedova E. Carpal Tunnel Syndrome Is an Early Unrecognized Feature of Rheumatoid Arthritis: A Population-Based Study [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/carpal-tunnel-syndrome-is-an-early-unrecognized-feature-of-rheumatoid-arthritis-a-population-based-study/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/carpal-tunnel-syndrome-is-an-early-unrecognized-feature-of-rheumatoid-arthritis-a-population-based-study/