Session Information
Date: Saturday, November 12, 2022
Title: Vasculitis – ANCA-Associated Poster I: Epidemiology, Outcomes, and Classification
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
Background/Purpose: Several studies have reported that patients with ANCA-associated vasculitis (AAV) are at increased risk of cardiovascular complications from accelerated atherosclerosis with an excess cardiovascular (CV) risk of 65%. HTN and diabetes mellitus (DM) are two of the most reported treatment-related complications observed at long-term follow-up. However, the risk of CV disease is greater in AAV and cannot be explained through traditional CV risk factors alone. ANCA are harmful antibodies that are directly involved in blood vessel damage through neutrophil and complement cascade activation, but it is unclear if they are directly responsible for the higher rate of CV complications in AAV. Therefore, we aimed to compare ANCA-associated and non-ANCA-associated vasculitis and their associations with mortality and CV outcomes.
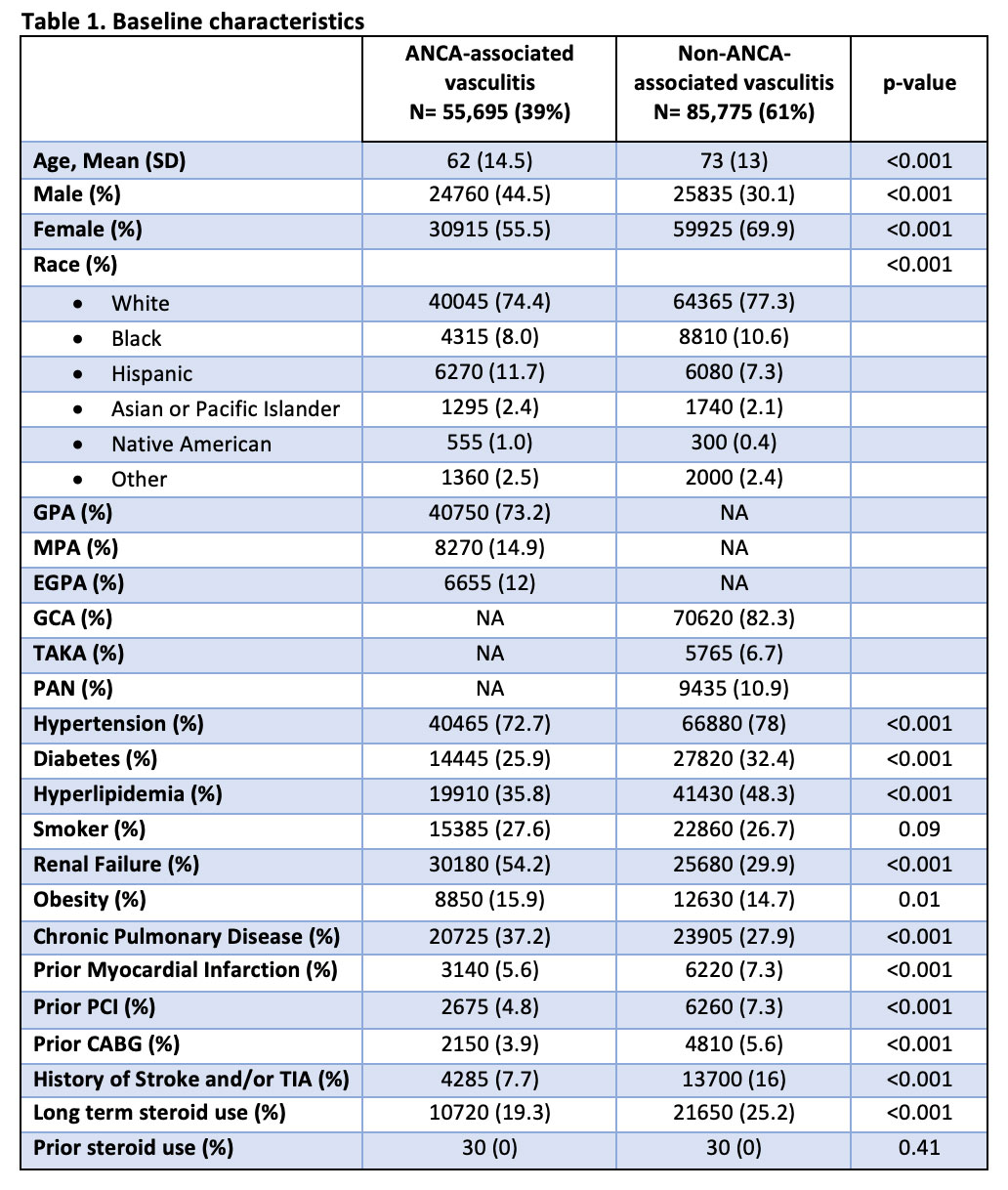
Methods: In this retrospective cohort study, we identified patients with ANCA-associated and non-ANCA-associated vasculitis based on ICD-10 codes, using the Nationwide Inpatient Sample database (NIS) from 2016 to 2019. We included all-cause mortality, atrial fibrillation (Afib), ST-elevation (STEMI) and non-ST elevation myocardial infarction (NSTEMI), heart failure (HF), cerebrovascular accident (CVA), and peripheral arterial disease (PAD) as our outcomes of interest. We implemented logistic regression analysis in the univariable and multivariable models. In the multivariable model, we adjusted all outcomes for potential confounders, including age, sex, ethnicity, obesity, anemia, diabetes, hypertension, renal failure, history of smoking or alcohol abuse, prior history of MI, primary coronary intervention (PCI), or coronary artery bypass grafting (CABG), coagulopathy, liver disease, chronic pulmonary disease, ischemic cardiomyopathy, Elixhauser comorbidity index, hypothyroidism, cancer, history of defibrillator or pacemaker, and long-term use of steroids, anticoagulants, antiplatelet or antithrombotic agents. The analysis was done using the STATA software, version 17.0 (SE).<
Results: We identified 141,470 patients with vasculitis, of whom 55,695 (39%) had AAV and 85,775 (61%) had non-ANCA associated vasculitis. Our results showed that patients with AAV had a higher mortality (OR: 1.17; 95%-CI 1.00-1.37; p-value = 0.045) when compared to patients with non-ANCA associated vasculitis even after adjusting for potential confounders. There was no difference in risk of ACS between the two groups (OR: 0.88; 95%-CI 0.75-1.03; p-value = 0.12). AAV was associated with a lower risk of Afib (OR: 0.74; 95%-CI 0.68-0.81; p-value < 0.001), HF (OR: 0.65; 95%-CI 0.60-0.71; p-value < 0.001), CVA (OR: 0.57; 95%-CI 0.51-0.64; p-value < 0.001) and PAD (OR: 0.56; 95%-CI 0.50-0.62; p-value < 0.001) when compared with patients with non-ANCA vasculitis.
Conclusion: Patients with AAV had a higher risk of in-hospital mortality. However, patients with non-ANCA vasculitis had a higher prevalence of Afib, ACS, HF, CVA, and PAD which may be related to their older age and larger vessel involvement. These results suggest that ANCA antibodies alone are not responsible for increased CV disease in this population.

To cite this abstract in AMA style:
Arevalo A, Shah P, Zala H, Haddadin F, Majmundar M, Ramirez Gomez A. Cardiovascular Burden in Patients with ANCA-Associated and Non-ANCA Associated Vasculitis [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/cardiovascular-burden-in-patients-with-anca-associated-and-non-anca-associated-vasculitis/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/cardiovascular-burden-in-patients-with-anca-associated-and-non-anca-associated-vasculitis/