Session Information
Session Type: Poster Session B
Session Time: 9:00AM-10:30AM
Background/Purpose: Uncontrolled inflammation in rheumatoid arthritis (RA) patients increases the risk for incident Ischemic Heart Disease (IHD) and venous thromboembolic (TE) events. Reducing inflammation using advanced therapies (AT) such as JAK inhibitors or anti-TNF drugs is expected to reduce these risks. Understanding the incidence of IHD and TE events before and after advanced therapy (AT) initiation may help clarify whether some ATs have specific toxicities or are relatively less protective. Clinical registries are best for precise observations on diagnosis, reasons for drug use and withdrawal, and disease activity. Administrative health databases are more comprehensive for comorbidities.
Methods: USRAT Registry combines administrative and clinical data. Our team is the single one treating rheumatology patients from our catchment area (about 500,000 people), while all their inpatient episodes are recorded in the administrative system of one single multisite hospital. Since 2003, we developed a registry of 1800+ patients treated with AT. All episodes of inpatient care for these patients were extracted from our hospital’s database from 1995 up to the end of 2021. Clinical charts were revised to confirm diagnosis and disease activity over time. We report severe IHD and TE events occurring over the 3 years before and the 3 years after initiation of a first AT in the RA patients whose chart revision is currently completed. We first analyzed data according to use of a single AT only (First) versus at least one drug switch over the 3-year period (Switch). We also isolated a subset of First patients who stopped their first AT but did not switch (First-Stop) from those remaining on first AT (Persistent).
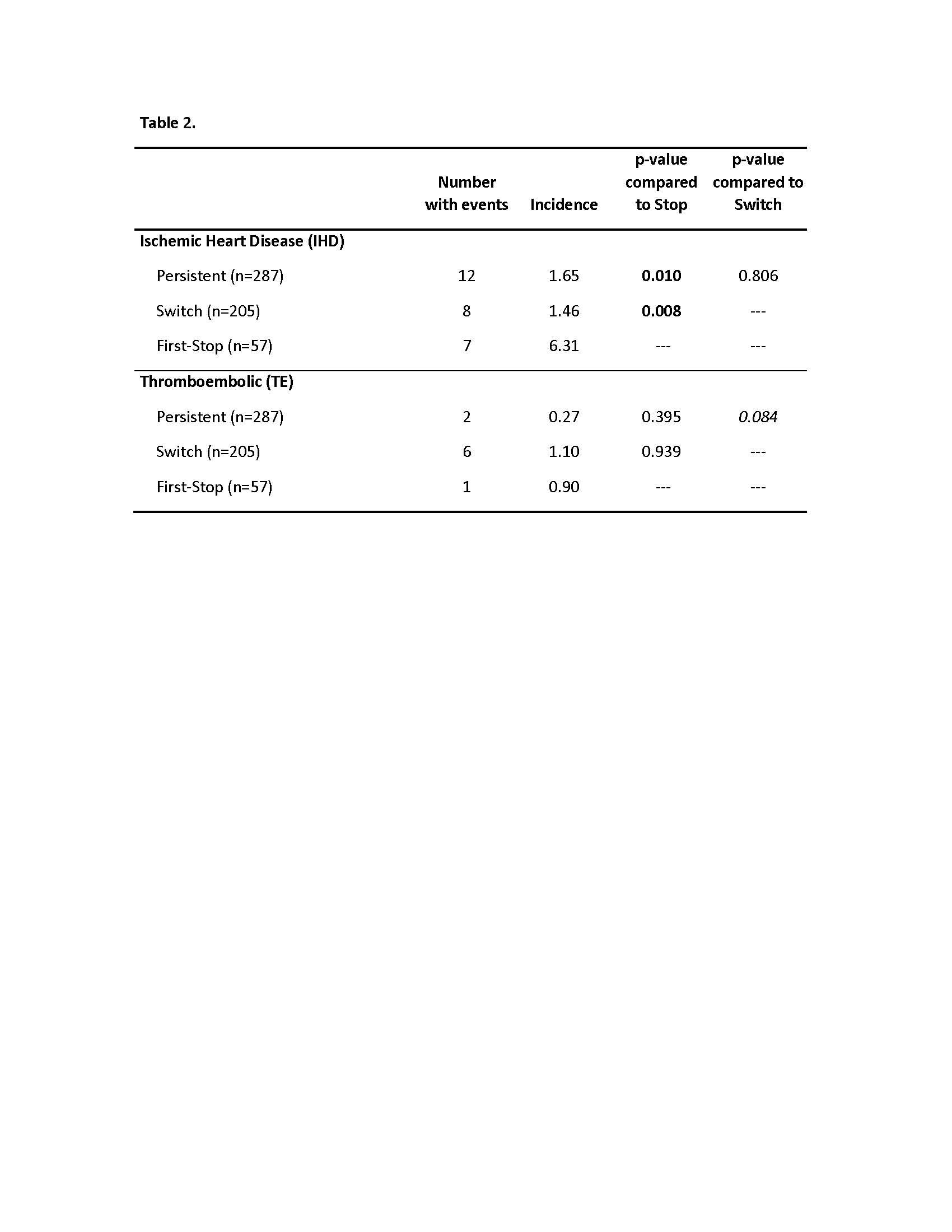
Results: Among patients labeled RA on the AT reimbursement form, RA was confirmed in 549 (65.8% women; mean age 59.3); mean disease duration 6.9 years at first AT initiation (71.4% anti-TNF). After first AT initiation (1386 patient-years), at least one IHD or TE event occurred in 27 (4.9%) and 9 (1.7%) patients, respectively (Table 1). Unexpectedly, a not significant increase in the 3-year incidence of IHD and TE events was seen following the start of a first AT. Incidence of IHD and TE events before AT was similar among Persistent, Switch and First-Stop groups. IHD incidence post-AT was not significantly different between First and Switch patients (Table 1). However, IHD post-AT was significantly more frequent in First-Stop than in Persistent or Switch patients (Table 2). Several First-Stop patients developed drug toxicity or severe comorbidities but most had other reasons to stop. There was a trend for fewer TE events in Persistent relative to Switch or First-Stop patients (p=0.08) (Table 2).
Conclusion: Prescribing an AT in patients with active RA may not be sufficient to bring their 3-year risk for IHD and TE events below their pre-AT levels. Switching had a neutral association with IHD relative to Persistence but may increase TE risk, suggesting a more direct role of persistent inflammation in TE. The worst outcomes were seen in patients who stopped their first AT and did not switch (First-Stop) over 3 years. Whether the more at risk First-Stop patients may be identified before AT initiation remains to be determined.

To cite this abstract in AMA style:
Carrier N, Roux S, Allard-Chamard H, Boire G. Cardiovascular and Thromboembolic Events in Rheumatoid Arthritis Patients Before and After Initiation of a First Advanced Therapy. Data from the University of Sherbrooke Registry of Advanced Therapies (USRAT) [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/cardiovascular-and-thromboembolic-events-in-rheumatoid-arthritis-patients-before-and-after-initiation-of-a-first-advanced-therapy-data-from-the-university-of-sherbrooke-registry-of-advanced-therapies/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/cardiovascular-and-thromboembolic-events-in-rheumatoid-arthritis-patients-before-and-after-initiation-of-a-first-advanced-therapy-data-from-the-university-of-sherbrooke-registry-of-advanced-therapies/