Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: The Weight-loss and Exercise for Communities with Arthritis in North Carolina (WE-CAN) trial was a community-based, pragmatic randomized clinical trial in men and women aged 50 years or older with symptomatic knee osteoarthritis and overweight or obesity. It established the efficacy of diet and exercise interventions on reduction in pain from knee osteoarthritis over 18 months (PMID 36511925). Previous studies noted depression and MJOA are associated with increased pain from knee osteoarthritis. This secondary analysis aimed to determine whether depressive symptoms and multiple joint osteoarthritis (MJOA) at baseline were associated with knee pain response in all WE-CAN trial participants.
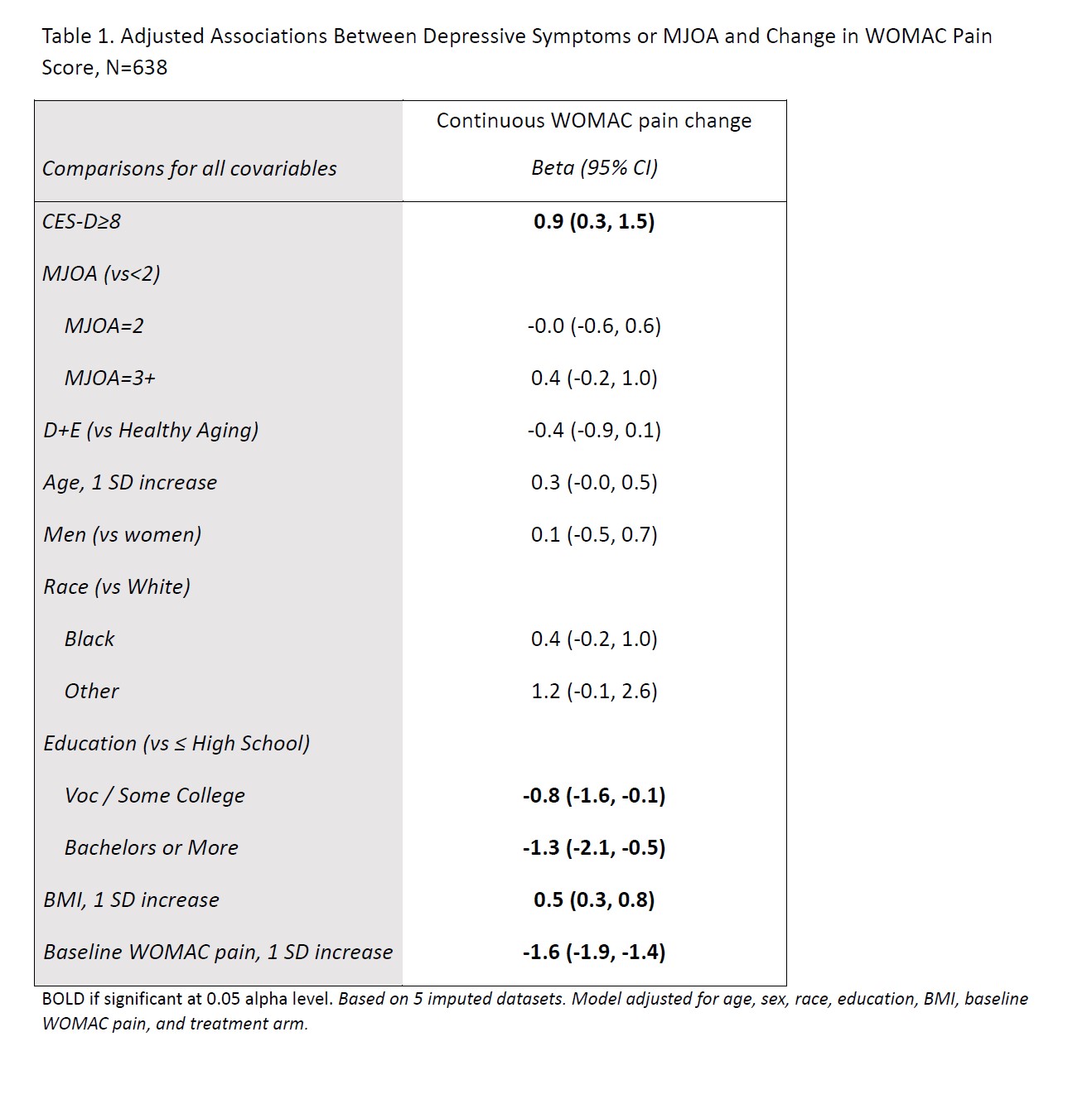
Methods: WE-CAN participants with WOMAC pain score available at 18-month follow-up, 10 item Centers for Epidemiological Studies Depression Scale (CES-D-10), and MJOA available at baseline defined the sample. Depressive symptoms were defined as a CES-D-10 score ³ 8, and MJOA as 2 or more joint types (knees, hips, fingers, spine, ankles, or other) from “self-reported arthritis of any joint” in the medical history questionnaire. Multiple linear regression was used to model change in WOMAC pain score (on 0-20 scare, minimum clinically important difference 1.6) adjusting for clinically relevant covariables including age, sex, race (White, Black, or Other), education (High School or less, Voc / Some College, or Bachelors or More), BMI, baseline WOMAC score, and treatment arm (Diet and Exercise or Successful Aging) to produce betas (β) and 95% confidence intervals (95% CI) for depressive symptoms and MJOA.
Results: Overall, 638 WE-CAN participants had complete data for this analysis (23.4% Male, 69.6% White, mean age 65.2 +/-7.7, mean BMI 36.3 +/- 6.4, and 51.3% in D+E group). Of these, 160 (25%) participants had a CES-D-10 score ³8, and 318 (50%) participants reported pain in ³2 joint types. Depressive symptoms were significantly associated with a worsening in WOMAC pain of 0.9 (0.2-1.6) from baseline to follow-up (Table 1). The confidence interval for this change in WOMAC pain includes the MCID of 1.6. There was no evidence of an association between MJOA and change in WOMAC pain.
Conclusion: Participants in the WE-CAN trial with depressive symptoms at baseline, but not MJOA, were found to have higher WOMAC pain scores at follow-up. These results denote the importance of depressive symptoms screening as those participants may not have comparable benefits from interventions. Further investigation of interventions targeting depression in addition to diet and exercise may offer additional benefit to patients with symptomatic knee OA and depressive symptoms.
To cite this abstract in AMA style:
Allcott N, Messier S, Mihalko S, Katz J, DeVita P, Hunter D, Quandt S, Alvarez C, Callahan L, Nelson A. Association of Depressive Symptoms and Multiple Joint Osteoarthritis with Pain Outcomes in the WE-CAN Trial [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/association-of-depressive-symptoms-and-multiple-joint-osteoarthritis-with-pain-outcomes-in-the-we-can-trial/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/association-of-depressive-symptoms-and-multiple-joint-osteoarthritis-with-pain-outcomes-in-the-we-can-trial/