Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Knee osteoarthritis (OA) and type 2 diabetes (T2D) commonly coexist, but their combined impact on health-related quality of life (HRQoL) remains understudied. Our objective was to assess the relationship between symptomatic knee OA (yes/no) and HRQoL in persons with type 2 diabetes and, if a relationship was found, to determine if it is due to depressed mood, sleep disturbance, fatigue, and/or walking limitation, which we hypothesized could be explanatory factors.
Methods: We conducted a secondary analysis of a cross-sectional study of individuals with T2D recruited from endocrinology clinics at three academic hospitals in Canada. Participants completed standardized online questionnaires that assessed sociodemographic factors, comorbidities to calculate the Functional Comorbidity Index (FCI), depressed mood (PROMIS Depression 8b), sleep disturbance (PROMIS Sleep Disturbance 4a), fatigue (PROMIS Fatigue 4a), walking limitation (Health Assessment Questionnaire walking difficulty item), HRQoL (EQ-VAS, 0–100), and joint symptoms. Symptomatic knee OA was defined using NICE criteria (age ≥45 years, activity-related knee pain, morning stiffness ≤30 minutes; no inflammatory arthritis). Linear regression modelled associations between knee OA and HRQoL, adjusting for age, gender, BMI, education, and comorbidities. The explanatory effects of sleep disturbance, depressed mood, and mobility limitation were assessed via sequential adjustment.
Results: Our study included 341 participants. Mean age was 66.4 (SD 9.7) years, 51.9% were women, 80.1% had post-secondary education, mean BMI was 29.1 (SD 6.7) kg/m², and 99 (29.0%) fulfilled NICE criteria for symptomatic knee OA (Table 1). Median HRQoL (EQ-VAS) was 68/100 (IQR 50, 80), with lower scores reported by individuals with knee OA (median 54 vs. 70). Compared to those without OA, participants with knee OA had worse sleep, fatigue, depressive symptoms, and higher rates of walking limitation (p < 0.0001 for all). After adjustment for age, gender, BMI, education, and comorbidities, the presence of symptomatic knee OA remained associated with lower HRQoL (β = −8.33, 95% CI: −12.72 to −3.94). Model performance improved with sequential adjustment, with adjusted R² increasing from 0.068 in the unadjusted model to 0.381 in the final model. The association was fully attenuated in the final model including sleep, mood, and walking limitation (β = −3.46, 95% CI: −7.63 to 0.71) (Figure 1).
Conclusion: Symptomatic knee OA is strongly associated with impaired HRQoL in T2D, explained by sleep disturbance, low mood, and mobility limitation. Integrated care addressing OA may improve quality of life in this population.
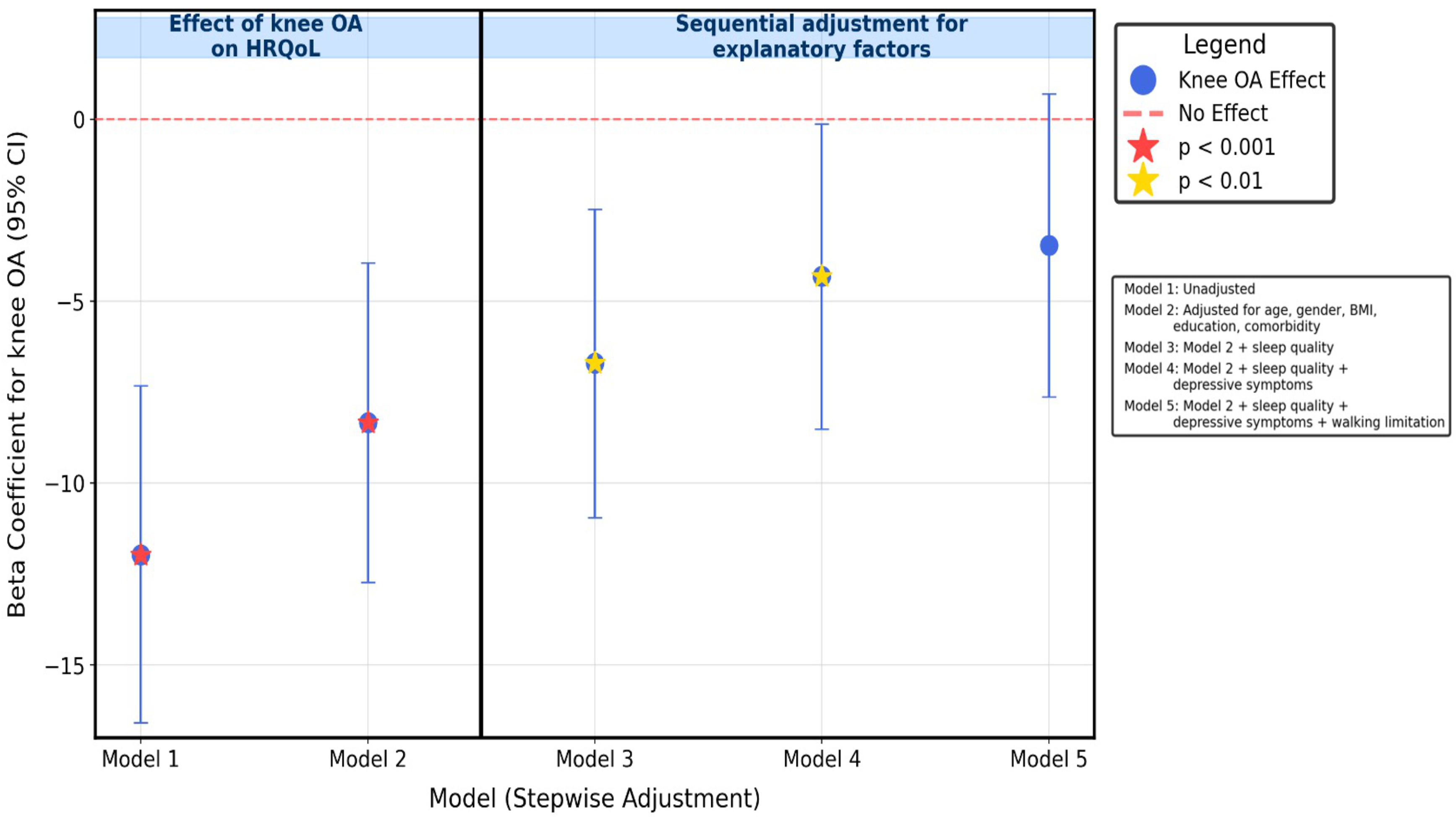 Figure 1: Linear regression modeling demonstrating the association between knee osteoarthritis and health-related quality of life before and after adjusting for potential confounders and sequential adjustment for potential explanatory factors.
Figure 1: Linear regression modeling demonstrating the association between knee osteoarthritis and health-related quality of life before and after adjusting for potential confounders and sequential adjustment for potential explanatory factors.
.jpg) Table 1. Characteristics of participants by symptomatic knee osteoarthritis status (N = 341)
Table 1. Characteristics of participants by symptomatic knee osteoarthritis status (N = 341)
To cite this abstract in AMA style:
Almodahka A, Weisman A, Shah B, Watson T, stanaitis I, Parikh A, Goldberg R, Lipscombe L, Hawker G, King L. Association Between Symptomatic Knee Osteoarthritis and Health-Related Quality of Life in Individuals with Type 2 Diabetes: A Cross-Sectional Study [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/association-between-symptomatic-knee-osteoarthritis-and-health-related-quality-of-life-in-individuals-with-type-2-diabetes-a-cross-sectional-study/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/association-between-symptomatic-knee-osteoarthritis-and-health-related-quality-of-life-in-individuals-with-type-2-diabetes-a-cross-sectional-study/