Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: Little is known of the association between pain threshold and knee/hip symptoms as well as radiographic knee/hip osteoarthritis (rOA). These analyses: 1) determined the association between pain threshold and presence of knee/hip symptoms or knee/hip rOA, 2) determined the association between pain threshold and the number of joints with knee/hip symptoms or rOA and 3) determined if associations differed by demographic or clinical characteristics.
Methods: Dolorimeter measurements for pain threshold were available for 1,602 participants returning for second follow-up (2008-11) in the Johnston County Osteoarthritis Project. Participants mean age was 67.9 (SD 9.0), 67.2% female, 31.0% African American, mean body mass index (BMI) 31.5 (SD 7.1) and a mean Center for Epidemiologic Studies Depression (CES-D) Scale score of 31.5 (SD 7.1). Pain threshold measurements were averaged (mean of 3.6kg ((SD 0.7)) over three trials from left and right trapezius muscles. Knee and hip OA were both defined by a Kellgren-Lawrence score of 2-4. Knee and hip symptoms were obtained at clinical interview with “on most days do you have pain, aching or stiffness in at least one knee/hip?“. Associations were determined with logistic regression while adjusting for age, race, BMI, CES-D scores and presence of hip or knee rOA. Interactions between pain threshold and clinical and demographic characteristics were tested at p<0.05.
Results: Knee and hip rOA were present in 45.7% and 40.3% of participants, respectfully. Knee and hip symptoms were present in 38.4% and 29.3% of participants, respectfully. A 1-unit increase in pain threshold was significantly associated with symptoms in the knee (adjusted odds ratio [aOR] 0.64 ((95% CI 0.54, 0.76)) and hip (aOR 0.67 ((95% CI 0.57, 0.79)). The figure illustrates the associations between pain threshold and number of knees and hips with symptoms. Compared to those without knee or hip symptoms, those with higher pain threshold were 20% less likely to have 1 joint with symptoms and 50% less likely to have 4 joints with symptoms. No significant associations were found with increased pain threshold and presence of knee or hip rOA or number of joints with knee and hip rOA. No significant interactions were found between pain threshold and demographic or clinical characteristics.
Conclusion: Participants with higher pain threshold were less likely to report knee and hip symptoms, an association that strengthened with the number of symptomatic joints. In contrast, no association was found with increased pain threshold and knee or hip rOA. These findings suggest the presence of knee or hip rOA may not be informative in understanding an individual’s knee or hip symptoms or useful for evaluating the efficacy of treatments targeting symptoms.
Figure. Associations between pain threshold and number of knees and hips with symptoms*.
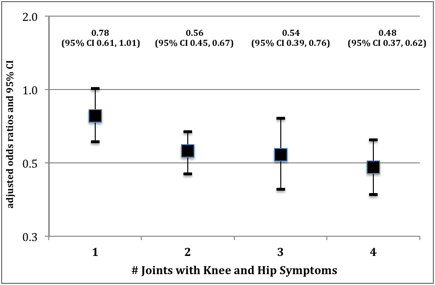
* referent = those with no knees or hips with symptoms
Disclosure:
A. P. Goode,
None;
X. A. Shi,
None;
J. Renner,
None;
R. Gracely,
None;
M. Maleki-Fischbach,
None;
J. M. Jordan,
Algynomics, Inc. ,
1,
Johnson and Johnson,
5,
Johnson & Johnson,
2,
Interleukin Genetics, Inc. ,
5,
Eli Lilly and Company,
5,
Mutual Pharmaceutical Company,
5.
« Back to 2012 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/association-between-pain-threshold-symptoms-and-radiographic-knee-and-hip-osteoarthritis-the-johnston-county-osteoarthritis-project/