Session Information
Date: Tuesday, November 14, 2023
Title: (1895–1912) Measures & Measurement of Healthcare Quality Poster II
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Research databases are missing 25-50% of race and ethnicity, typically related to Black and Hispanic data.1,2The absence of this data can lead to inaccurate assessment of patient outcomes by race.1,3,4 Our aim is to assess the impact of missing race and ethnicity on outcome measures in a JIA registry (Pediatric Care Outcomes Improvement Network (PR-COIN)).
Methods: Descriptive analysis of demographic and clinical data from 9 PRCOIN centers was performed. Missing race and ethnicity data was quantified by site. Relative risk (RR) of moderate to severe clinical juvenile arthritis disease activity score (cJADAS ³5) at first visit after enrollment was compared across race (Black, White, other, missing) and ethnicity (Hispanic, non-Hispanic, missing).A RED Cap survey on data collection and entry was administered to each site.
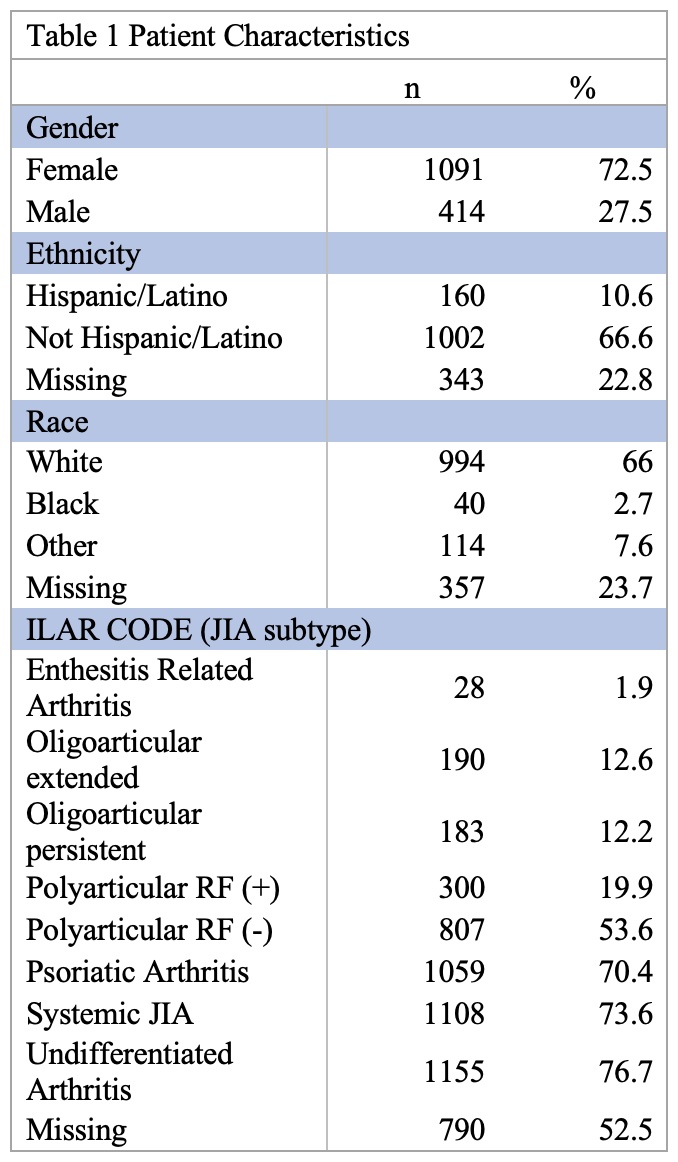
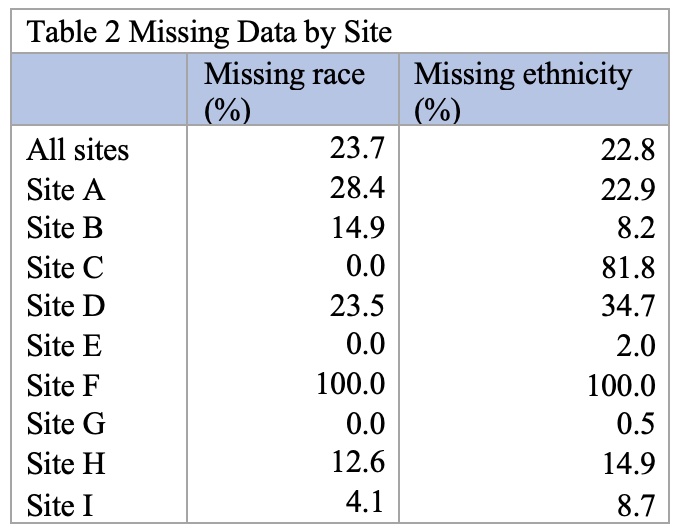
Results: A total of 1,505 JIA patients from 9 (of 23) sites were included (Table 1). Race was missing for 24% and ethnicity was missing for 23% with missing data ranging from 0-100% (Table 2).
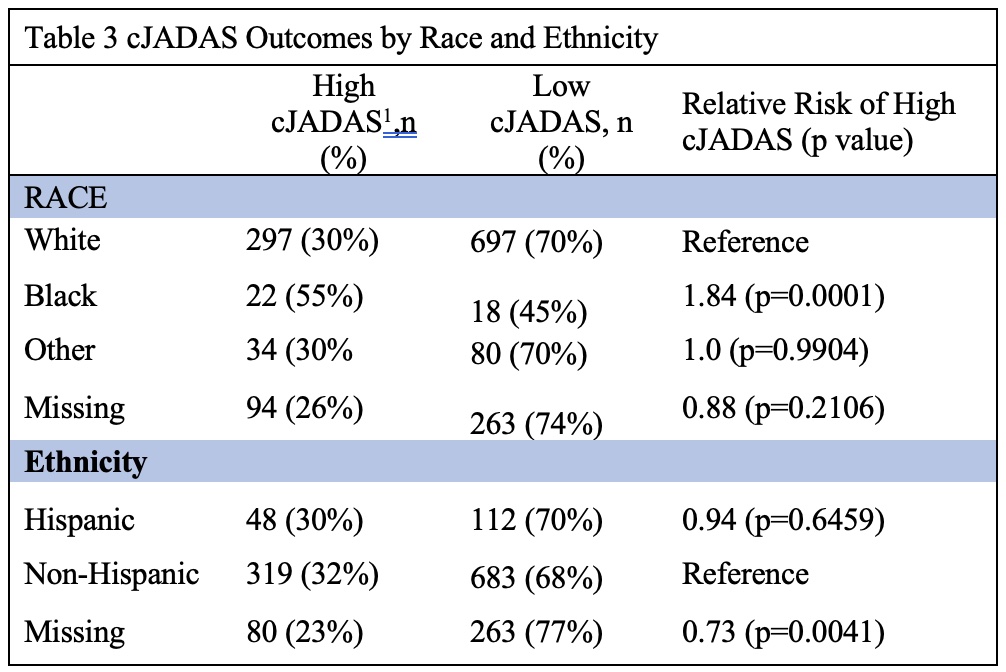
CJADAS score at first follow-up (2-6 months after enrollment) was high (³5) for 30% of White patients and 55% of Black patients with a RR of 1.84 (p=0.0001) of higher cJADAS in Black patients (Table 3). There was no difference in risk for patients of Other races, relative to White patients, RR 1.0 (p=0.99). For patients missing race, risk of high cJADAS at first follow-up was lower than for White patients, RR 0.88 (p=0.21). There was no difference in rates of high cJADAS at first follow up by Hispanic vs non-Hispanic ethnicity, RR 0.94 (p=0.65). For patients with missing ethnicity, risk of high cJADAS at first follow-up was 27% lower than non-Hispanic patients, RR 0.73 (p=0.0041).
Four of 9 sites completed a survey. Two sites are missing 0% of race and < 2% of ethnicity data. One is missing 12.6% race and 14.9% ethnicity. These 3 sites enter data manually. One is missing 100% of race and ethnicity data and uploads data via electronic data transfer (EDT).
Conclusion: Amount of missing race and ethnicity data is highly variable, ranging from 0-100%. Additional survey data is needed to understand the impact of data entry method on missingness. Preliminary, unadjusted analysis suggests RR of high cJADAS at first follow up is higher for Black compared to White patients in a setting of missing data. Patients with missing race had lower RR of high cJADAS at first follow up compared to White patients. This suggests that completion of missing race could change RR assessments. Next steps include multivariate analysis to adjust for confounding factors (age, gender, site, ILAR code, insurance status).It also includes interventions to complete missing data and reassessment of RR of high cJADAS.
To cite this abstract in AMA style:
Banschbach K, Singleton J, Morgan E, Wang X. Assessing Disparities Through Missing Race and Ethnicity Data: Results from a Juvenile Arthritis Registry [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/assessing-disparities-through-missing-race-and-ethnicity-data-results-from-a-juvenile-arthritis-registry/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/assessing-disparities-through-missing-race-and-ethnicity-data-results-from-a-juvenile-arthritis-registry/