Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Interstitial lung disease (ILD) is a serious complication of SSc and inflammatory myopathy (IM), necessitating accurate and early detection for improved outcomes. Lung ultrasound (LUS) is a potential alternative to computed tomography (CT) for ILD screening. We previously developed interpretation criteria for LUS ILD detection (LUS-ILD-20 and 24 criteria) showing high accuracies. Our current study aimed to test whether convolutional neural networks (CNNs) could accurately detect ILD and its severity, and understand their agreement with, and added benefit to, human interpretation.
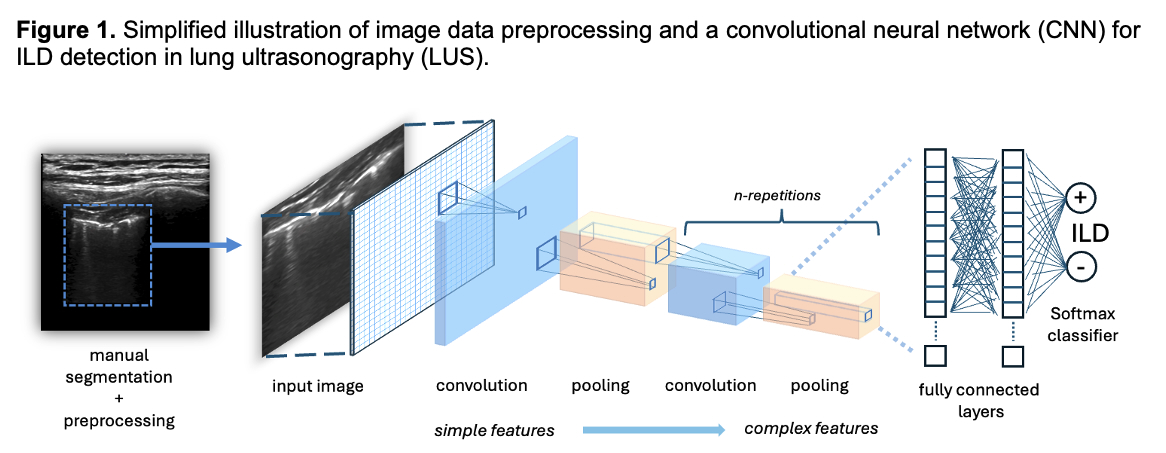
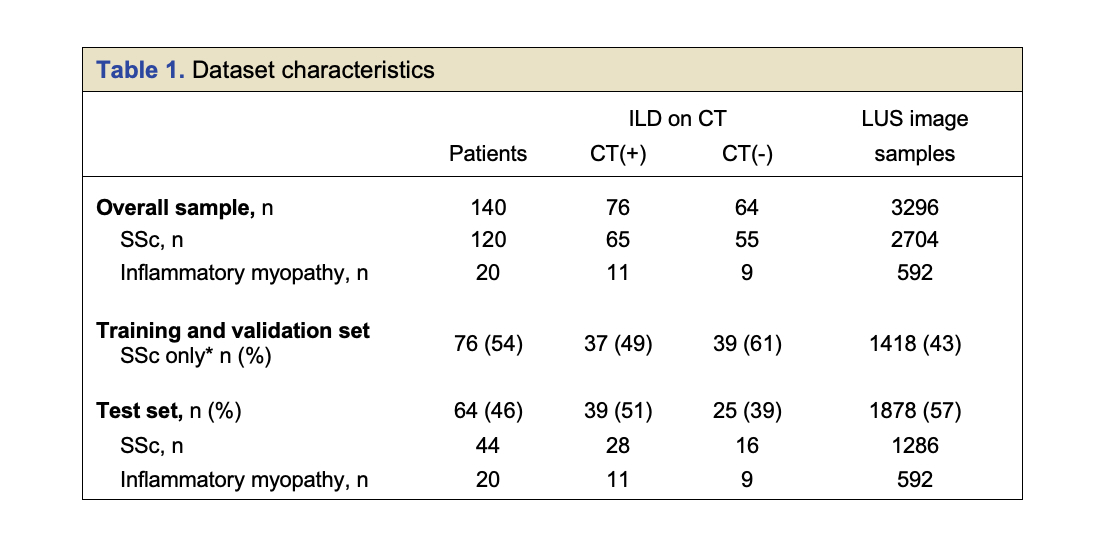
Methods: All patients meeting ACR criteria for SSc and randomly selected patients meeting ACR criteria for IM enrolled in our prior LUS studies who underwent LUS cine imaging of 14 lung zones and CT imaging were included (140 patients) (Table 1). For each lung zone, two images were extracted and preprocessed. Data were separated into a training set, labelled as ILD(+/-) using LUS-ILD-24 (1418 images), and an unlabeled test set (1878 images). Several CNN architectures (InceptionV1, VGG-16, and ResNet50) were trained using transfer learning and fine-tuning techniques. We also developed a novel and more efficient CNN (LUS-Net) (Figure 1). CNN performance for ILD detection was evaluated using the test set on: 1) individual lung zone images, and 2) per patient, using summed prediction scores across lung zones. Sensitivity, specificity, receiver operator curves (ROC), and Cohen’s kappa were assessed. Spearman correlation results between each CNN and measures of severity were evaluated, including CT lung pathology quantification using Computer-Aided Lung Informatics for Pathology Evaluation and Ratings (CALIPER), pulmonary function testing (PFT) indices, and LUS-ILD-24 severity.
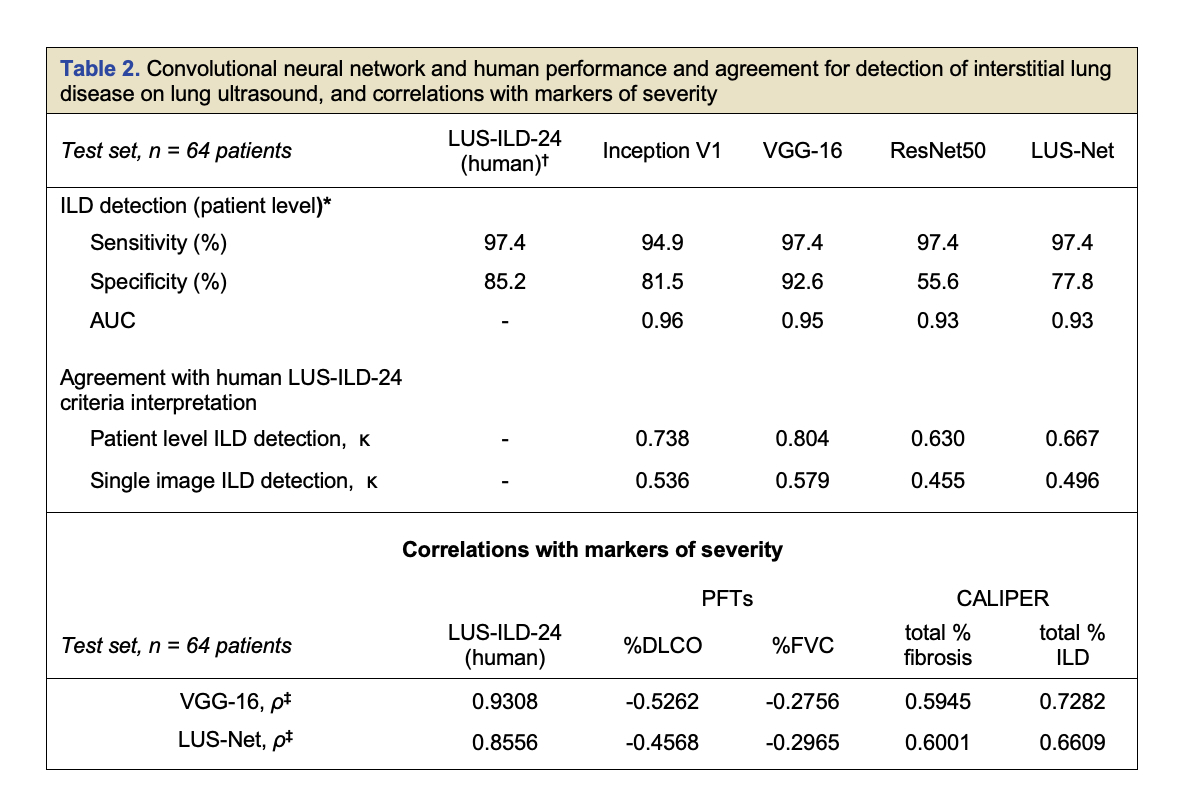
Results: ILD(+) per CT in the test set of 64 patients was detected by the CNNs with sensitivities and specificities ranging from 93% to 97% and 62% to 91%, respectively (Table 2). Human LUS-ILD-24 showed 97% sensitivity and 85% specificity. Area under the ROC curve for CNNs ranged from 0.93 to 0.96. LUS-ILD-24 and CNNs’ study interpretation showed substantial agreement (κ = 0.63 – 0.80). VGG-16 and LUS-Net showed the best CNN ILD screening performance. VGG-16, LUS-Net and LUS-ILD-24, all identified one identical case as a false negative; CT in this patient showed trace focal reticulation. Significant correlations were observed between CNNs and LUS-ILD-24 severity (very strong), PFT indices (FVC: weak, DLCO: moderate), and CALIPER CT quantification (strong). Combining human and CNN interpretation did not result in improved accuracy.
Conclusion: We trained several state-of-the-art and a novel CNN on a large LUS database in SSc and IM, which showed excellent performance in ILD detection. VGG-16 and the smaller novel LUS-Net performed similarly compared to human interpretation. Combining human and CNN interpretation provided no additional benefit, however in real world use, this may vary based on the experience of the human interpreter. Overall, CNN interpretation alone or in combination with human reading may provide increased confidence and reproducibility to enable LUS to replace CT in ILD screening in select populations.
To cite this abstract in AMA style:
Fairchild R, Mar D, Deluna M, Baker M, Tamang s, Guo H, Fiorentino D, Chung L. Artificial Intelligence Assisted Interpretation of Lung Ultrasound Imaging for the Detection of Interstitial Lung Disease [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/artificial-intelligence-assisted-interpretation-of-lung-ultrasound-imaging-for-the-detection-of-interstitial-lung-disease/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/artificial-intelligence-assisted-interpretation-of-lung-ultrasound-imaging-for-the-detection-of-interstitial-lung-disease/