Session Information
Date: Sunday, November 17, 2024
Title: Abstracts: RA – Diagnosis, Manifestations, & Outcomes III: Best Day (RA Subpopulations)
Session Type: Abstract Session
Session Time: 3:00PM-4:30PM
Background/Purpose: Earlier diagnosis and treatment of Rheumatoid Arthritis (RA) improve patient outcomes including pain, disability and overall mortality (NICE, 2024). The National Institute for Health and Care Excellence (NICE) in the United Kingdom (UK) has set a target for those with suspected early inflammatory arthritis to be assessed in a Rheumatology clinic within three weeks (NICE, 2024). The National Early Inflammatory Arthritis Audit (NEIAA) gathers data assessing this target. In 2023, this target was met for 38% nationally, and for only 10% within our trust, Gloucestershire Hospitals NHS Foundation Trust (GHNFT) (NEIAA, 2023). Low initial diagnostic accuracy (50% in our sample) once seen in the Rheumatology clinic further delays reaching an accurate final diagnosis.
Novel methods are required to supplement the scheduling and diagnostic systems currently used in clinical practice. Locally, GHNFT requests serological data at the point of referral, but this is not used to inform decisions about prioritising patients for review. Nationally, the NEIAA has gathered service-level data including serological tests and final diagnoses for almost a decade. In combination, there is scope to use these data to develop an artificial intelligence (AI) algorithm that both prioritises patients at highest risk of RA for early Rheumatology review, and for making a more accurate initial diagnosis. We collaborated with colleagues at Princeton University to develop such an algorithm, using neural nets (NN).
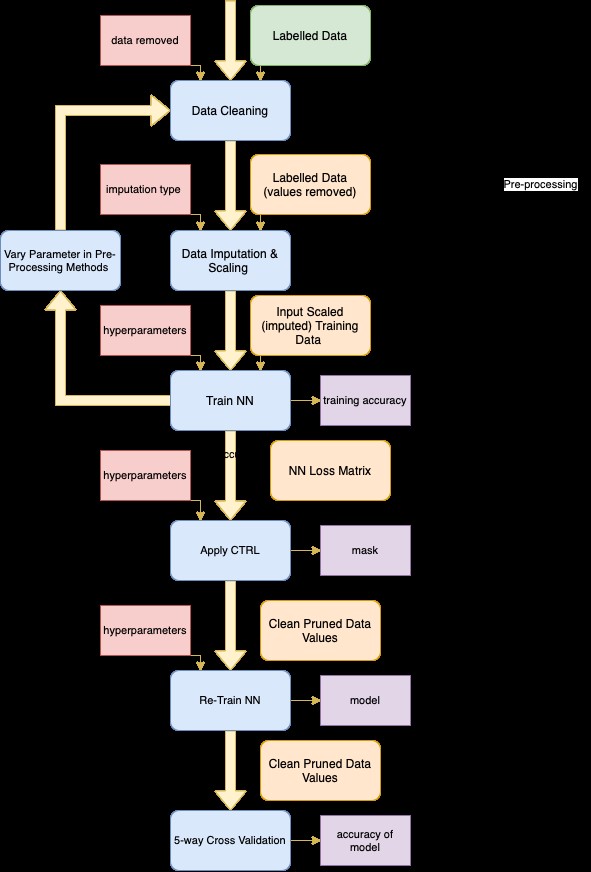
Methods: Our NN was trained on cleaned, formatted, anonymised serological data of a sample of 1000 patients from the GHNFT, gathered over the past 18 months. We used a unique technique of clustering training losses for label error detection to remove mislabelled data from our dataset and increase accuracy. The data was labelled with a 4-tier diagnosis system: 1 = confirmed EIA, 2 = possible EIA, 3 =low possibility of EIA, and 4 =not EIA. All patient identifiers were removed before being sent outside of the NHS.
Our NN had architecture 5-32-4, batch size 10 over 1000 epochs. We trained on 1-4 tiered labels and binarised labels (0-1 scale: 0 = not EIA, previously 2, 3 & 4, 1=definitely EIA, previously 1).
Results: A 50.9% accuracy was achieved for the 4-tier labels and 87.6% for binary labels, using 5-way cross validation. Scheduling, highlighted as key usage for the algorithm, showed a predicted 41.6% improvement in a KPI of waiting times for high-risk patients.
Conclusion: We have developed an AI algorithm that promises to aid in both scheduling more timely appointments for high-risk patients, and increasing diagnostic accuracy once seen in the Rheumatology service. As large volumes of data are already routinely collected by NEIAA, there is further scope to train the neural nets to align clinical practices with the national quality standards set by NICE. Implementation would begin with a small-scale regional pilot programme to test economic and clinical viability, ensuring that all stakeholders are consulted throughout; as such a transformative change will undoubtedly require taking into account a myriad of ethical and political considerations.
To cite this abstract in AMA style:
Ahmed U, Kalap K, Johnson H. Artificial Intelligence: A Novel Tool in the Belt for Improving Rheumatoid Arthritis Outcomes in the National Health Service, United Kingdom [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/artificial-intelligence-a-novel-tool-in-the-belt-for-improving-rheumatoid-arthritis-outcomes-in-the-national-health-service-united-kingdom/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/artificial-intelligence-a-novel-tool-in-the-belt-for-improving-rheumatoid-arthritis-outcomes-in-the-national-health-service-united-kingdom/