Session Information
Date: Saturday, November 12, 2022
Title: Vasculitis – Non-ANCA-Associated and Related Disorders Poster I: Giant Cell Arteritis
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
Background/Purpose: Most previous studies have demonstrated a similar overall survival in patients with GCA compared to the background population. However, we have previously reported an increased mortality during the first two years after diagnosis in patients diagnosed through 2010, in particular among those aged < 70 years. Up till now, no data on cause of death has been presented from our area. Our aim was to investigate all-cause and cause-specific mortality in a large population-based cohort of patients with temporal artery biopsy-proven GCA (TAB+GCA) compared to matched controls from the general population.
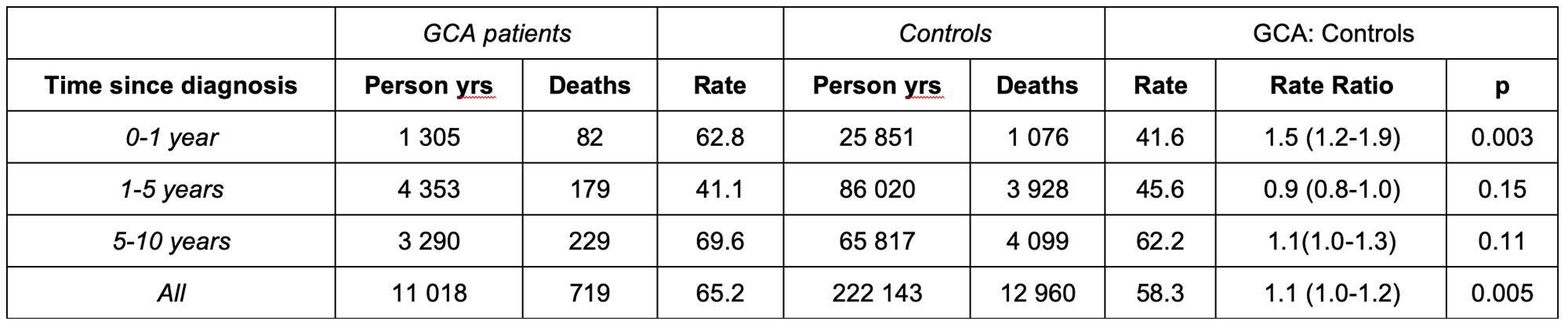
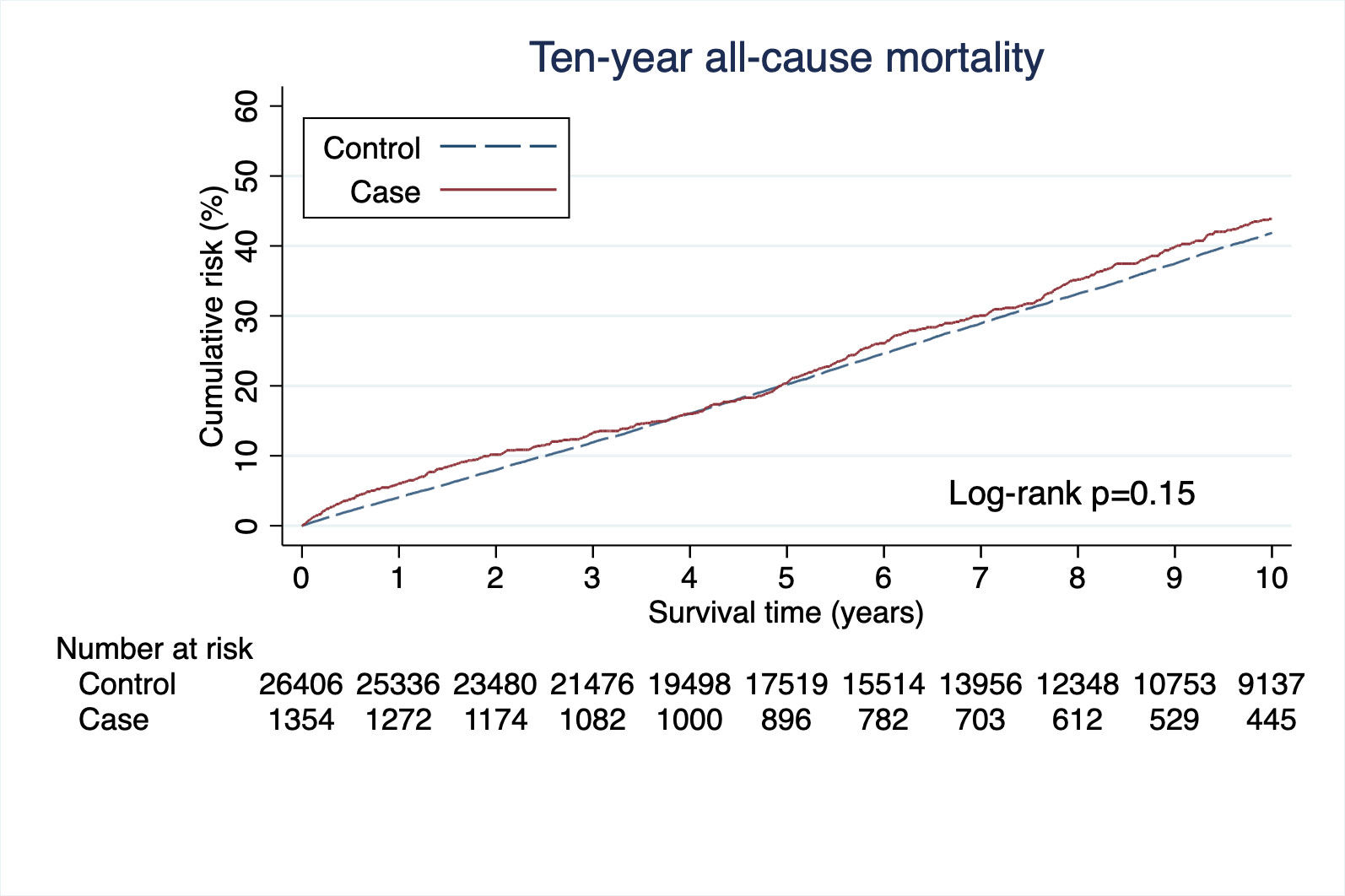
Methods: All patients diagnosed with TAB+GCA between 1997 and 2019 in the region were included in this study. For each patient with GCA, 20 controls were selected from the background population matched for age, sex, and place of residency. Controls with a vasculitis diagnosis were excluded. Data on all-cause mortality were extracted from the national cause of death register. Time of follow up was calculated in person-years (py) from the date of GCA diagnosis for cases (index-date for controls) to death or end of study (December 31, 2020). Rates of death for patients and controls were calculated and rate ratios (death rate in GCA: controls) were estimated. Survival was also studied using the Kaplan-Meier curves. Differences between groups were studied using the Log-Rank test. Primary cause of death was grouped into the following categories: vasculitis, infection, cardiovascular, cancer and other.
Results: A total of 1,354 patients (71% female) with TAB+GCA and 26,406 controls were included. The mean age at diagnosis was 75.2 (SD 7.9) for all patients, 75.5 (SD 7.6) for females vs. 74.5 (SD 8.4) for males. Seven hundred nineteen patients with GCA died during 11,018 py of follow up vs. 12,960 controls during 222,143 py of follow up. The rate of death was 65.3/1,000 py in GCA patients vs. 58.3/1,000 py in controls resulting in a rate ratio of 1.1 (95% CI 1.0-1.2). During the first year after GCA diagnosis (index-date) the rate ratio was 1.5 (95% CI 1.2-1.9). The death rate and rate ratios for different time periods after GCA diagnosis (index date) are summarized in Table 1. The 1, 5 and 10-years cumulative survival was 94%, 79% and 56% in patients and 96%, 80% and 58% in controls (p = < 0.01), Figure 1. During the first year from diagnosis, the main cause of death was cardiovascular disease (Table 2). By contrast, a smaller proportion of patients with GCA died from cancer compared to controls.
Conclusion: In this study, mortality in patients with GCA was increased with 50% compared to matched controls during first year of follow up after diagnosis. The main cause of this early excess mortality appears to be cardiovascular disease.

To cite this abstract in AMA style:
Sode J, Rathmann J, Wilding A, Turesson C, Mohammad A. All-Cause and Cause-Specific Mortality in Giant Cell Arteritis, a Population-based Study [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/all-cause-and-cause-specific-mortality-in-giant-cell-arteritis-a-population-based-study/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/all-cause-and-cause-specific-mortality-in-giant-cell-arteritis-a-population-based-study/