Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Older age is a recognized risk factor for serious infection (SI) associated with anti-TNF therapy in rheumatoid arthritis (RA). Among older adults with RA, one-third are diagnosed after age 60 (late-onset RA, LORA), while others are diagnosed earlier in life (young-onset RA, YORA). LORA is characterized by a more acute disease onset and higher inflammatory burden, potentially due to age-related immune dysregulation. However, it is unclear whether RA onset age independently influences infection risk associated with TNF initiation in older adults. This study examines SI risk in older adults with LORA versus YORA initiating anti-TNF therapy.
Methods: Using the FORWARD-The National Databank for Rheumatic Diseases data from 2001-2019, we studied RA patients aged ≥60 years who started anti-TNF therapy. Patients were categorized as LORA or YORA based on their age at RA diagnosis (≥60 or < 60 years) and propensity-matched on age at anti-TNF initiation, sex, race/ethnicity, Medicare coverage, comorbidities, and HAQ-disability scores. Those with other rheumatic diseases, cancer, or HIV before the first SI were excluded. Anti-TNF initiation was identified when patients not using anti-TNF at enrollment reported its use at subsequent biannual visits. SI was defined as infection requiring IV antibiotics, hospitalization, or resulting in death and was attributed to anti-TNF if it occurred during treatment or within three months of discontinuation. Patients were censored at the end of TNF treatment plus 3 months (to account for SI risk window), death, or the end of the study. Kernel propensity-matched survival analyses estimated the risk difference of SI between LORA and YORA.
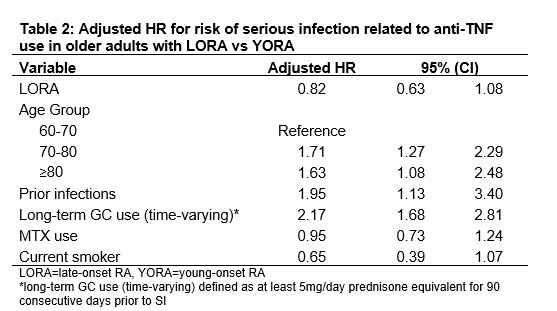
Results: 1219 LORA patients were matched to 6030 weighted YORA patients. At baseline, LORA patients had shorter RA disease duration and fewer prior infections but were more likely to be current smokers and to use concomitant MTX compared to YORA patients. All other baseline variables were well-balanced (Table 1). During follow-up, the crude incidence of SI was 34.2 per 1000 patient-years in LORA patients and 27.9 per 1000 patient-years in YORA patients. After kernel propensity matching, the risk of SI did not significantly differ between LORA and YORA (HR 0.89, 95% CI 0.60-1.34). In Cox regression analyses with GC use treated as a time-varying variable, the risk of SI increased 1.6 to 1.7-fold with older age at TNF initiation, 1.9-fold with prior infection, and 2.2-fold with recent long-term GC use (Table 2).
Conclusion: The risk of SI did not differ between LORA and YORA, indicating that age at RA onset alone does not significantly impact infection risk associated with TNF initiation in older adults. Although older age at treatment initiation was associated with increased SI risk, it should not deter anti-TNF use, as appropriate treatment can substantially improve RA outcomes. Prior infection and recent long-term GC use were also independently associated with SI risk, emphasizing the importance of minimizing GC exposure and implementing infection prevention strategies to mitigate risk and optimize outcomes in older adults initiating TNF therapy.
.jpg)
To cite this abstract in AMA style:
Lee J, Pedro S, Michaud K. Age of Disease Onset and Risk of Serious Infection with anti-TNF Use in Older Adults with Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/age-of-disease-onset-and-risk-of-serious-infection-with-anti-tnf-use-in-older-adults-with-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/age-of-disease-onset-and-risk-of-serious-infection-with-anti-tnf-use-in-older-adults-with-rheumatoid-arthritis/