Session Information
Date: Sunday, November 13, 2022
Title: SLE – Diagnosis, Manifestations, and Outcomes Poster II: Manifestations
Session Type: Poster Session C
Session Time: 1:00PM-3:00PM
Background/Purpose: The reasons for the high cardiovascular morbidity in patients with SLE are not fully understood. Here, we combine a mendelian randomization (MR) approach and investigation of a clinical SLE cohort to evaluate the contribution of SLE-genetic risk to the development of myocardial infarction (MI).
Methods: 1028 patients with SLE from Norway and Sweden who fulfilled ≥4 ACR-82 (96%), ACR-97 (98%) or SLICC2012 (94%) classification criteria were included in the study. Clinical data was collected from medical charts and patients were genotyped using the Global Screening Array (Illumina). Using the NHGRI-EBI GWAS catalog, established, independent SLE risk SNPs (p< 5e-8) were selected and summary statistics for coronary artery disease (CAD) and MI were identified for each of these SNPs using the MR Base version of the catalog. MR was conducted using four conventional MR methods, including the MR Egger method, on the largest available dataset using a strict definition of MI (ncases=11,622, ncontrols=187,840).
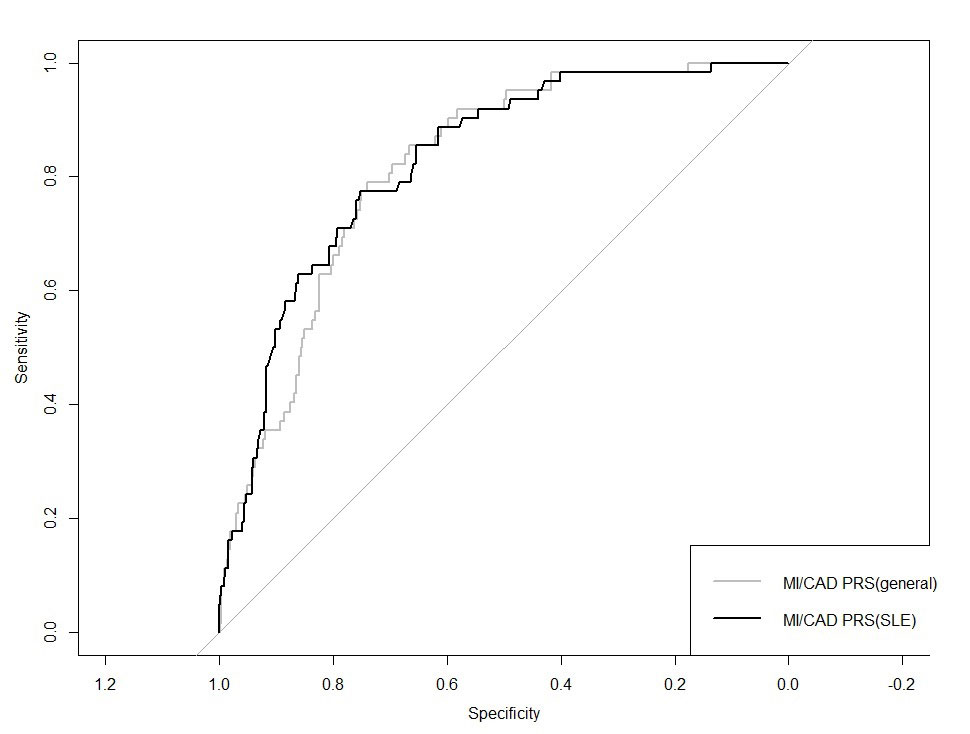
Next, an SLE CAD/MI polygenic risk score (CAD/MI PRSSLE) was calculated for each patient with SLE in our cohort based on 14 SLE risk SNPs associated with CAD/MI in the datasets. A second PRS (CAD/MI PRSgeneral) based on 44 established CAD/MI SNPs (p< 5e-8) regardless of association with SLE, was constructed and the predictive abilities of the two scores combined with the age at follow-up were evaluated by comparing the areas under the receiver operating characteristics (ROC) curves (AUCs). Patients with a high or low CAD/MI PRS, defined as having a score in the highest or lowest quartiles, were compared using logistic regression, adjusting for the age at follow-up, age at SLE onset and gender.
Results: The MR analysis revealed a significant association between the genetic risk of SLE and MI using the MR Egger method (OR 1.07 (1.02-1.13, p< 0.01). The association was robust to outliers and pleiotropy and consistent across the investigated MR methods. No influence by confounding factors such as hypertension, smoking, alcohol consumption or hyperlipidemia was identified.
In the clinical cohort, 62 patients (7.7%) had experienced at least one MI, with a mean age at the first MI of 60 years. Patients with a high CAD/MI PRSsle (14 SNPs) displayed a three-fold higher risk of MI (OR 3.04 (1.43−6.49), p< 0.01) compared with patients with a low CAD/MI PRS. No associations were found between the CAD/MI PRSsle and smoking, hypertension, hyperlipidemia or the presence of anti-phospholipid antibodies (all p >0.05). In a multivariable model, both the CAD/MI PRSsle (p< 1×10-04) and CAD/MI PRSgeneral (p< 0.01) were significantly associated with MI. In the ROC curve analysis, the CAD/MI PRSsle and CAD/MI PRSgeneral displayed similar predictive abilities of MI (AUC 0.83 and AUC 0.82, respectively, pcomparison=0.52), figure 1.
Conclusion: A high genetic risk of SLE is associated with an increased risk of myocardial infarction and may be an equally important contributor as established CAD/MI SNPs to the risk of MI in patients with SLE.
To cite this abstract in AMA style:
Reid S, Sandling J, Pucholt P, Sayadi A, Sjöwall C, Lerang K, Jönsen A, Bengtsson A, Molberg Ø, Rudin A, Rantapää-Dahlqvist S, Ronnblom L, Leonard D. A High Genetic Risk of SLE Is Associated with an Increased Risk of Myocardial Infarction; A Combined Observational and Mendelian Randomization Study [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/a-high-genetic-risk-of-sle-is-associated-with-an-increased-risk-of-myocardial-infarction-a-combined-observational-and-mendelian-randomization-study/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-high-genetic-risk-of-sle-is-associated-with-an-increased-risk-of-myocardial-infarction-a-combined-observational-and-mendelian-randomization-study/