Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: IgG4-related disease (IgG4-RD) is a fibro-inflammatory disorder that can affect nearly any organ. Because of the often tumefactive nature of IgG4-RD and its typical organ involvement (e.g., pancreas, salivary glands, lymph nodes), patients may be misdiagnosed with malignancy. This impacts quality of life and contributes to illness-related uncertainty, even after diagnosis. Patients’ worry and fear about cancer are also driven by conflicting evidence regarding the associations of IgG4-RD with malignancy. A better understanding of cancer in patients with IgG4-RD is important for counseling patients and guiding management after the diagnosis of IgG4-RD. We sought to characterize: (1) the frequency with which patients with IgG4-RD have been mistakenly told that they had cancer; and, (2) the development of malignancy after IgG4-RD diagnosis.
Methods: Patients in a large center for IgG4-RD in the US were followed prospectively. All patients fulfilling the ACR/EULAR Classification Criteria for IgG4-RD were invited to complete a survey regarding their history of malignancy. They were asked if they had ever been told they had cancer, whether that diagnosis was ultimately proven to be IgG4-RD, and the details of any incident malignancy following the diagnosis of IgG4-RD. For deceased patients, the medical record was reviewed for a history of malignancy and, if present, details extracted. Malignancies were confirmed by review of pathology reports. Non-melanoma skin cancers were not considered in this analysis.
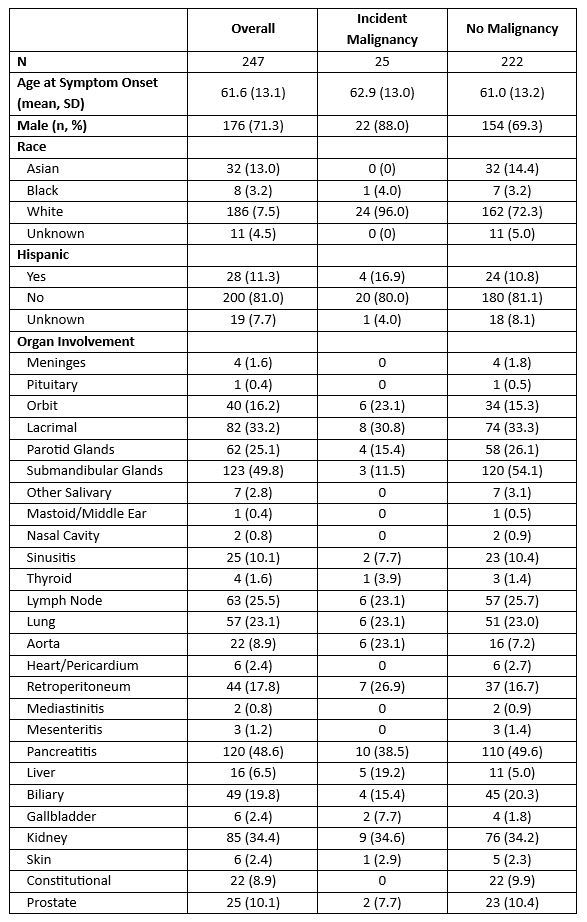
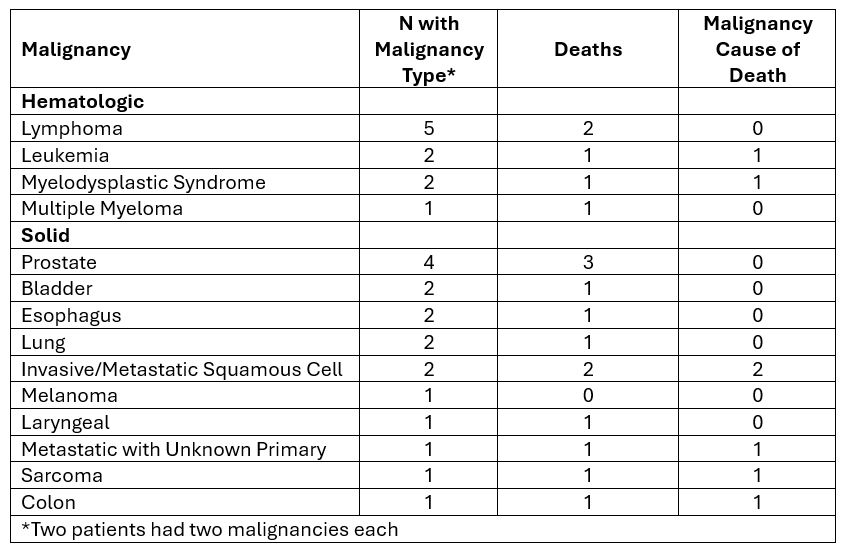
Results: Of 348 patients who fulfilled the ACR/EULAR Classification Criteria, 317 were alive and sent surveys; 216 (68.1%) responded. 31 of 348 were deceased. We included n=247 who were survey responders or were deceased with medical record reviewed (Table 1). Among survey responders, 8 (3.7%) were given false diagnosis of cancer on their journey to an IgG4-RD diagnosis. Over a mean follow-up of 5.5 (SD 4.0) years, 25 (10.1%) patients had an incident malignancy (incidence rate: 1.83 / 100 patient years, 95% CI 1.2-2.7). Two patients had two malignancies (Table 2). The mean age at malignancy was 69.4 (11.6) years. Those with vs without malignancy had similar age of onset of IgG4-RD (62.9 vs 61.0 years) but were more often male (88.0% vs 69.3%, p=0.051) and White (96.0% vs 72.3%, p=0.01). Those with and without malignancy had similar organs affected by IgG4-RD except that submandibular gland involvement was substantially less common in malignancy than those without malignancy (3 [11.5%] vs 120 [54.1%], p< 0.0001). Lymphoma was the most common malignancy (5, 20%). The median (IQR) time from IgG4-RD symptom onset to malignancy was 4.6 (2.6, 8.2) years. Malignancy was the cause of death in 7 (22.6%) of those who died.
Conclusion: Nearly 5% of IgG4-RD patients were told that they had cancer before their IgG4-RD diagnosis was established. 10% of patients with IgG4-RD develop malignancy, most often lymphoma, a median of 5 years after IgG4-RD onset. The question of whether or not IgG4-RD is associated with an increased risk of cancer is associated with potential confounders and requires further study.
To cite this abstract in AMA style:
McMahon G, Jha I, Katz G, Perugino C, Fernandes A, Stone J, Wallace Z. A Contemporary Assessment of the Burden of Malignancy in IgG4-Related Disease [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/a-contemporary-assessment-of-the-burden-of-malignancy-in-igg4-related-disease/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-contemporary-assessment-of-the-burden-of-malignancy-in-igg4-related-disease/