Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Plasmapheresis (PLEX) has a compelling rationale in its ability to remove pathogenic ANCAs, in the management of ANCA-associated vasculitis (AAV), particularly in patients with severe manifestations such as diffuse alveolar hemorrhage (DAH). Despite its theoretical benefits, the role of PLEX in AAV + DAH remains debated, and inconsistent evidence regarding its long-term effects on mortality and organ function raises important questions. Our study aims to compare the risk of in-hospital mortality in patients with AAV + DAH who received PLEX to those who did not, seeking to clarify the role of PLEX in improving clinical outcomes and addressing current uncertainties regarding its efficacy in this context.
Methods: Using the National Inpatient Sample database from January 2020 to December 2022, we extracted data on AAV + DAH (AAVDAH), categorizing patients into two groups: those who received plasmapheresis (AAVDAHpl) and those who did not (AAVDAH). We analyzed key demographic, clinical, and hospital-related factors, including gender, age, race, Charlson Comorbidity Index (CCI), income, payer, region, and bed size. The primary outcome was in-hospital mortality, with secondary outcomes including LOS, total charges, sepsis, mechanical ventilation, and pressor requirements. Adjusted odds ratios for mortality and complications were calculated using logistic regression.
Results: A total of 1,470 AAVDAH patients were identified, with 375 receiving PLEX (AAVDAHpl). The mean age was 54.45 years in the AAVDAH group and 56.65 years in the AAVDAHpl group. Regarding comorbidity burden (CCI), 25.85% of AAVDAH patients had moderate, compared to 24.00% in AAVDAHpl, and 38.78% had severe burden, compared to 45.33% in AAVDAHpl. AAVDAHpl patients were more likely to be admitted to hospitals in the Northeast (32.00% vs. 19.05%) (Table 1). The mean LOS was significantly longer in the AAVDAHpl group (23.59 days) vs. 13.79 days (p < 0.001), and total charges were higher ($424,256.7 vs. $220,514.1, p < 0.001). The odds of death in the AAVDAHpl group was 1.99 (95% CI: 1.03 - 3.85) (p = 0.0415). Significant associations were found between PLEX and various complications, including sepsis (OR = 2.08, p = 0.041), mechanical ventilation (OR = 4.82, p < 0.001), and pressor requirement (OR = 5.04, p < 0.001). RPGN was significantly associated with PLEX (OR = 4.06, p = 0.0044) (Fig 1). Adjusted analyses revealed that mechanical ventilation, sepsis, and pressor requirement were strongly associated with increased mortality in the AAVDAHpl group (p < 0.001 for all), while RPGN was not statistically significant (p = 0.120) (Fig 2).
Conclusion: This study indicates that PLEX treatment in AAV + DAH may be linked to higher mortality and more severe complications, highlighting the need for a cautious and individualized approach to its use. However, our results are limited by the lack of data on other treatments received by patients for their AAV. The increased risk of complications associated with PLEX further complicates its role in management. Therefore, further research is essential to identify when PLEX is most beneficial, especially in patients with DAH, and to clarify its optimal application in clinical practice.
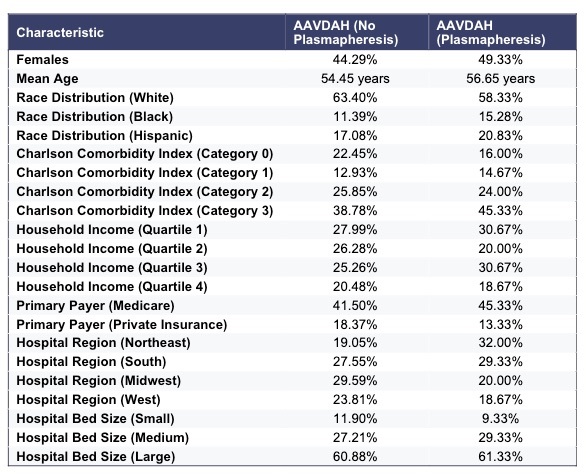 Figure 1: Odds ratios (ORs) with 95% confidence intervals (CIs) for outcomes comparing AAVDAH with plasmapheresis (AAVDAHpl) and AAVDAH without plasmapheresis.
Figure 1: Odds ratios (ORs) with 95% confidence intervals (CIs) for outcomes comparing AAVDAH with plasmapheresis (AAVDAHpl) and AAVDAH without plasmapheresis.
.jpg) Figure 2: Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) for mortality, adjusting for complications, in patients with AAVDAH who received plasmapheresis (AAVDAHpl).
Figure 2: Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) for mortality, adjusting for complications, in patients with AAVDAH who received plasmapheresis (AAVDAHpl).
.jpg) Table 1: Baseline Characteristics Comparison Between AAVDAH and AAVDAH with Plasmapheresis (AAVDAHpl).
Table 1: Baseline Characteristics Comparison Between AAVDAH and AAVDAH with Plasmapheresis (AAVDAHpl).
To cite this abstract in AMA style:
Pannala S, Rajamanuri M, Sama S, Saliba F, Mourad O, Sangaraju K, Katikineni V, Slobodnick A. Predictors for Mortality in Patients Who Received Plasmapheresis for Diffuse Alveolar Hemorrhage in ANCA-Associated Vasculitis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/predictors-for-mortality-in-patients-who-received-plasmapheresis-for-diffuse-alveolar-hemorrhage-in-anca-associated-vasculitis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/predictors-for-mortality-in-patients-who-received-plasmapheresis-for-diffuse-alveolar-hemorrhage-in-anca-associated-vasculitis/