Session Information
Date: Tuesday, October 28, 2025
Title: (2052–2078) Muscle Biology, Myositis & Myopathies – Basic & Clinical Science Poster III
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Idiopathic inflammatory myopathies (IIMs) encompass a heterogenous group of autoimmune diseases characterized by inflammation of muscle and other target organs. Muscle biopsy was historically the gold standard to characterize these myopathies. With advances in serological, electrophysiological and imaging diagnostics for IIMs, the role of muscle biopsy in the evaluation of contemporary patients with suspected IIM is not clear. Here, we aim to evaluate current practice in the diagnosis of IIMs at an academic medical center with particular focus on characteristics of patients diagnosed with IIMs who underwent muscle biopsy versus those who did not and whether muscle biopsy changed diagnosis.
Methods: A retrospective cohort study of adult patients diagnosed with a primary IIM by a rheumatologist or neurologist at a tertiary care medical center was performed. Potential subjects were identified using ICD-10 codes. Demographic, serologic, imaging, histopathologic, and treatment data were collected. Patients were divided into two groups based on whether or not a muscle biopsy was performed. Demographic and clinical characteristics were initially analyzed using chi-squared tests and t-tests; adjusted logistic regression modeling was used to identify factors associated with performing muscle biopsy.
Results: A total of 150 patients with IIM were included, of which 103 patients (68.7%) underwent muscle biopsy and 47 patients (31.3%) who did not (Table 1). There were no significant differences in baseline clinical characteristics between the two groups. Muscle strength, myositis specific antibodies (MSA), gender and primary specialist (neurology vs rheumatology) were not significantly associated with biopsy performance. However, patients with positive HMG-CoA Reductase (HMGCR) antibodies were significantly less likely to have a biopsy (OR 0.2, p=0.02, Table 2). Time was also a significant factor associated with biopsy performance with lower odds of biopsy being performed in more recent years (OR 0.6, p=0.002, Figure 1). With regards to outcomes, the biopsy changed the diagnosis in only 13 cases (12.6%). Results of EMG (performed in over 85% in each group) and MRI (performed in less than 15% in each group) were not significantly associated with biopsy performance.
Conclusion: Our findings suggest a clear trend towards reduced biopsy use over time and whenever HMG-CoA reductase antibodies were present. When biopsies were performed, they infrequently changed the pre-biopsy diagnosis. Given a lack of change in diagnosis in most patients, it may stand to reason that muscle biopsy could be reserved for equivocal or atypical clinical presentations of myositis.
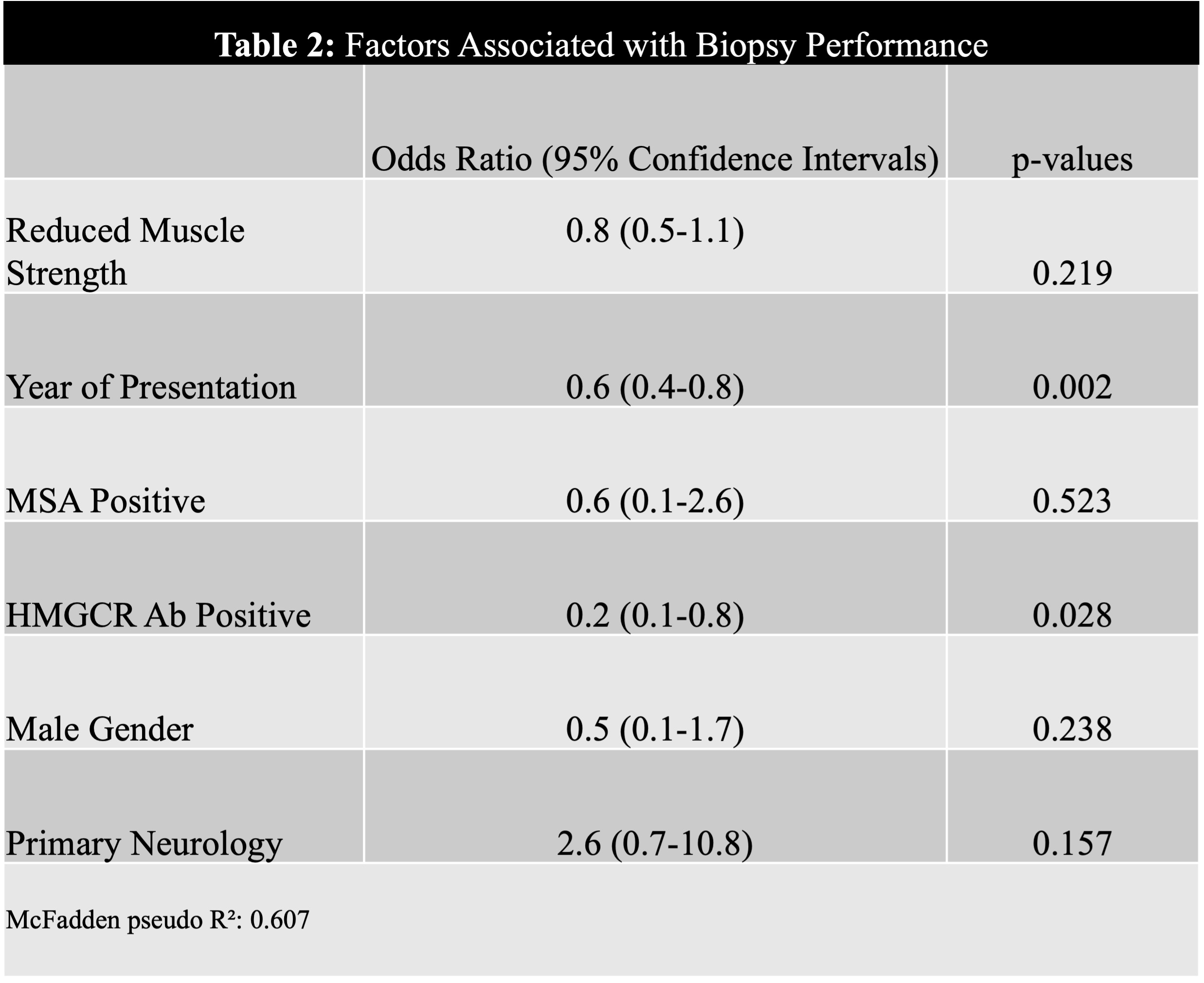
.jpg) Table 2: Factors Associated with Biopsy Performance
Table 2: Factors Associated with Biopsy Performance
 Figure 1: Line Graph Plot of Percentage of Biopsies Over Time
Figure 1: Line Graph Plot of Percentage of Biopsies Over Time
To cite this abstract in AMA style:
Purohit A, Shakoor N, Cherny D, Schmukler J. A Changing Paradigm: Reassessing the Role of Muscle Biopsy in Idiopathic Inflammatory Myopathies in a Single-Center Cohort [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/a-changing-paradigm-reassessing-the-role-of-muscle-biopsy-in-idiopathic-inflammatory-myopathies-in-a-single-center-cohort/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-changing-paradigm-reassessing-the-role-of-muscle-biopsy-in-idiopathic-inflammatory-myopathies-in-a-single-center-cohort/