Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Recent studies have demonstrated that patients with RA are at an increased risk for the development of lung cancer and lung cancer related death. However, the cause for the increased risks has not been established. Although previous studies have investigated the delay of other age recommended cancer screenings, few studies have investigated lung cancer screening in RA patients with a smoking history. Therefore, we evaluated the cumulative incidence of chest CT imaging in RA patients with either a current or former smoking history between 50-80 years old.
Methods: We performed a retrospective cohort study of patients with incident RA in a geographically defined area who fulfilled either the 1987 ACR or 2010 ACR/EULAR classification criteria between 2010 and 2019. Non-RA comparators of similar age, sex and county were randomly selected. The analyses included RA and non-RA patients who were between the ages of 50 and 80 years old and were either former or current smokers. Patients with a prior history of lung cancer were excluded from analyses. Chest CT imaging was defined as completed if it was performed by the end of the study period, emigration out of the geographical area, or death. Aalen-Johansen methods determined the cumulative incidence of chest CT imaging in both cohorts, accounting for the competing risk of death. Cox proportional hazard models adjusted for age, sex, index year, and education were utilized to compare the rates of chest CT imaging.
Results: This study included 407 patients with RA and 360 non-RA comparators. The patients with RA had a mean age of 63 years, 57% being female, and 52% having education beyond high school. During follow-up, >50% of the RA patients had chest CT imaging (55.8% [50.7-61.5]) compared to the non-RA cohort with < 40% (37.8% [32.3-44.2]) (Figure 1). After adjusting for age, sex, index year, and education, the patients with RA were 90% more likely to have chest CT imaging compared to the non-RA cohort (aHR 1.90 [1.51-2.39]. The increased likelihood of chest CT imaging persisted when examining former (aHR 1.95 [1.48-2.57]) and current (aHR 1.88 [1.23-2.89]) smokers separately.
Conclusion: RA was associated with an >85% increase in chest CT imaging after adjusting for potential confounders in this analysis of former and current smokers. These findings suggest that the increased risk of lung cancer related death in RA patients is not due to a decrease in chest CT imaging leading to a delay in the diagnosis of lung cancer. The increased incidence of chest CT imaging in the RA cohort could partially be explained by the increased risk of interstitial lung disease in those with RA, prompting more frequent evaluation of respiratory symptoms with chest CT imaging. Therefore, further studies investigating adherence to lung cancer screening guidelines, the effect of changes in lung cancer screening guidelines, and the impact of pack years are necessary to fully understand the impact of lung cancer screening on the RA population.
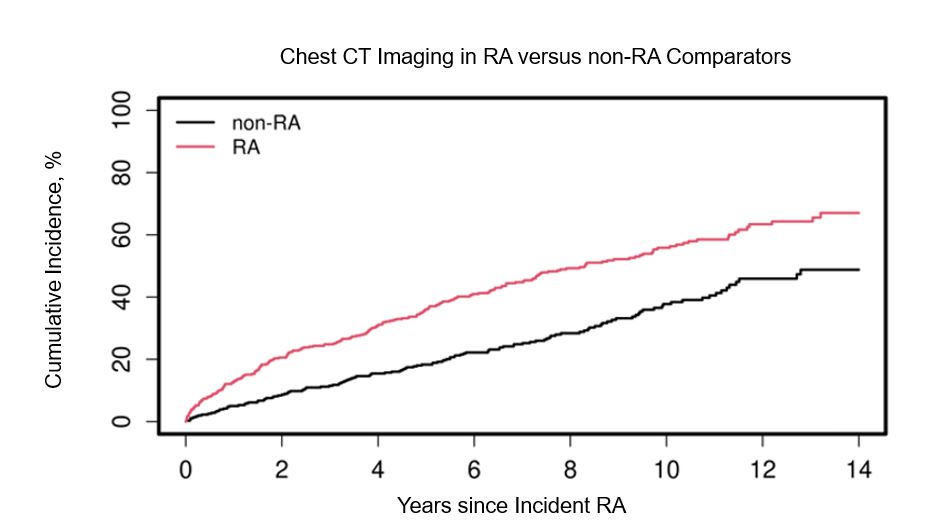 Figure 1. Cumulative Incidence of Chest CT Imaging in RA versus non-RA comparators
Figure 1. Cumulative Incidence of Chest CT Imaging in RA versus non-RA comparators
To cite this abstract in AMA style:
Brooks R, Achenbach S, Kronzer V, England B, Leasure E, myasoedova E, Davis J, Crowson C. Evaluating a Potential Cause of Excess Lung Cancer Mortality in RA: An Analysis of Chest CT Imaging Frequency in RA [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/evaluating-a-potential-cause-of-excess-lung-cancer-mortality-in-ra-an-analysis-of-chest-ct-imaging-frequency-in-ra/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/evaluating-a-potential-cause-of-excess-lung-cancer-mortality-in-ra-an-analysis-of-chest-ct-imaging-frequency-in-ra/