Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Systemic autoimmune rheumatic diseases (SARDs) are a group of autoimmune diseases that affect multiple organ systems, including the lungs. The development of interstitial lung disease (ILD) in the context of SARD (SARD-ILD) is a significant clinical concern due to its high prevalence, progressive nature, and its associated morbidity and mortality. There is limited published evidence describing how SARD-ILD patients with disease progression are being managed in the United States. This study aims to bridge the knowledge gap by describing the treatment patterns of patients with SARD-ILD following ILD progression.
Methods: This retrospective cohort study used Optum Clinformatics® administrative claims database from 01 January 2017 to 31 March 2024. The study cohort included adult patients diagnosed with SARD-ILD on or after 01 Jan 2018 and with evidence of ILD progression. Disease progression was identified using previously published claims-based proxies, which included health care utilization related to the management of ILD progression The earliest date of ILD progression was defined as the index date, with a requirement for a minimum of 12-month continuous enrollment before (baseline period) and after the index date (follow-up period). The proportion of patients receiving pharmacologic and non-pharmacologic treatments related to SARD-ILD following ILD progression was descriptively assessed for the overall SARD-ILD cohort. Pharmacologic treatments include antifibrotics, biologic and non-biologic disease modifying antirheumatic drugs (DMARDs), immunomodulators, oral corticosteroids, and other ILD-related treatments. Non-pharmacologic treatments included lung transplant, pulmonary rehabilitation and supplemental oxygen therapy.
Results: The study included a total of 6,431 patients. The mean (standard deviation [SD]) age of the overall cohort was 71.2 (11.1) years and 75.3% were female (Table 1). Rheumatoid arthritis was the most prevalent underlying SARD type (52.6%). The mean (SD) follow-up duration was 936 (467) days. While 83% of patients received any pharmacologic treatment group during the follow-up, only 55% have received disease modifying treatments (i.e., biologic and non-biologic DMARDs, immunomodulators, and antifibrotics). Oral corticosteroids and non-biologic DMARDs were the most frequently prescribed pharmacologic treatment groups (Figure 1). Among immunomodulators, mycophenolate (10.6%), azathioprine (5.5%), and tacrolimus (0.8%) were the most commonly prescribed medications. While only 3.5% of patients received antifibrotics after progression, we observed increasing trend in the use of antifibrotics across the study period. Supplemental oxygen therapy was the most commonly used non-pharmacologic treatment (Figure 1).
Conclusion: The study provides real-world insights into the treatment patterns of patients with SARD-ILD after ILD progression. The study findings suggest unmet needs and gaps in current treatment strategies remain. The limited use of disease modifying pharmacotherapies post-progression underscores a gap between real-world practice and evidence-based recommendations, potentially leading to suboptimal disease management.
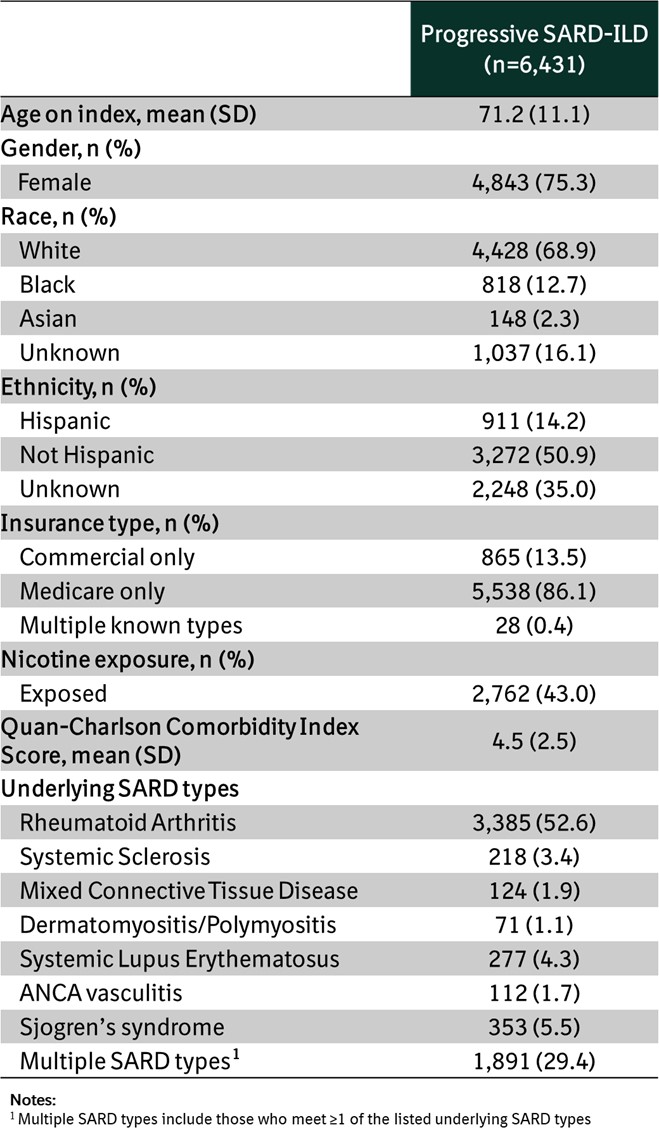 Table 1. Baseline demographics and clinical characteristics
Table 1. Baseline demographics and clinical characteristics
.jpg) Figure 1. Proportion of patients receiving ILD-related treatments after ILD progression during follow-up, among all patients with SARD-ILD
Figure 1. Proportion of patients receiving ILD-related treatments after ILD progression during follow-up, among all patients with SARD-ILD
To cite this abstract in AMA style:
Yang J, Sadowski K, Kharat A, Chauffe A, Kulkarni T. Real-World Treatment Patterns of Patients with Systemic Autoimmune Rheumatic Disease-associated Interstitial Lung Disease After Progression in The United States [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/real-world-treatment-patterns-of-patients-with-systemic-autoimmune-rheumatic-disease-associated-interstitial-lung-disease-after-progression-in-the-united-states/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/real-world-treatment-patterns-of-patients-with-systemic-autoimmune-rheumatic-disease-associated-interstitial-lung-disease-after-progression-in-the-united-states/