Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Idiopathic inflammatory myopathies (IIMs) are a heterogenous group of rare autoimmune inflammatory rheumatic diseases, including dermatomyositis (DM).
Methods: Data were drawn from the Adelphi Real World IIMs Disease Specific Programme™, a cross-sectional survey, including retrospective data collection, of rheumatologists, dermatologists, neurologists, and internists in Europe (France, Germany, the United Kingdom) and the United States (US) from September 2023–July 2024. Physicians reported demographics, consultation history, tests, and diagnoses, for up to 10 consecutively consulting adult patients with a physician-confirmed diagnosis of DM. Analyses were descriptive, and missing data were not imputed.
Results: Overall, 222 physicians provided data on 513 DM patients (n=381 Europe, n=132 US). Physician reported patient demographics at survey are reported in Table 1. Mean (standard deviation [SD]) patient age was 49.5 (12.8) years, 73% were female, and 87% were White. Mean [SD] time since DM diagnosis was 2.7 (2.9) years. Family history of an autoimmune disease was confirmed for 38% of patients and 67% had a confirmed comorbidity.Signs/symptoms present at onset included fatigue (63%; Europe 66%, US 53%), heliotrope rash (45%; Europe 46%, US 41%), Gottron’s papules (46%; Europe 48%, US 41%), erythematous rashes (without secondary changes) (40%; Europe 39%, US 42%), and myalgia 29%; Europe 29%, US 29%).Diagnostic characteristics are reported in Table 2. Mean (SD) time from symptom onset to diagnosis was 24.3 (32.4) weeks, and 13.1 (27.2) weeks from first consultation to diagnosis. Following DM symptom onset, 47% of patients initially consulted a general practitioner (GP)/ primary care physician (PCP), 22% consulted a dermatologist, and 14% consulted a rheumatologist. For patients who initially consulted a GP/PCP, dermatologist, or rheumatologist, the mean (SD) durations from first consultation to DM diagnosis were 12.4 (21.1), 8.1 (11.6), and 16.7 (33.4) weeks, respectively.Creatine kinase (CK) testing was conducted to aid diagnosis for 84% of patients and myositis specific/associated antibody testing for 74%. Overall, 34% of patients were initially diagnosed with a different condition, which was later identified as DM. Among these patients, initial diagnoses included 21% fibromyalgia, 20% systematic lupus erythematosus, and 16% rheumatoid arthritis (Table 2). Figure 3 shows the rate of initial diagnoses by physician types that conducted the first consultation. For patients that had been given an initial diagnosis, mean (SD) duration from first consultation to DM diagnosis was 18.2 (34.8) weeks (Europe 17.3 [27.4], US 19.7 [44.8]).
Conclusion: While almost half of patients first consulted a PCP, DM diagnosis was invariably made by a specialist. Despite significant levels of testing to aid diagnosis, other than CK, testing practice varies between patients but more generally between the US and Europe. Further research is needed to confirm the consequences of delay in terms of clinical and patient-reported outcomes.
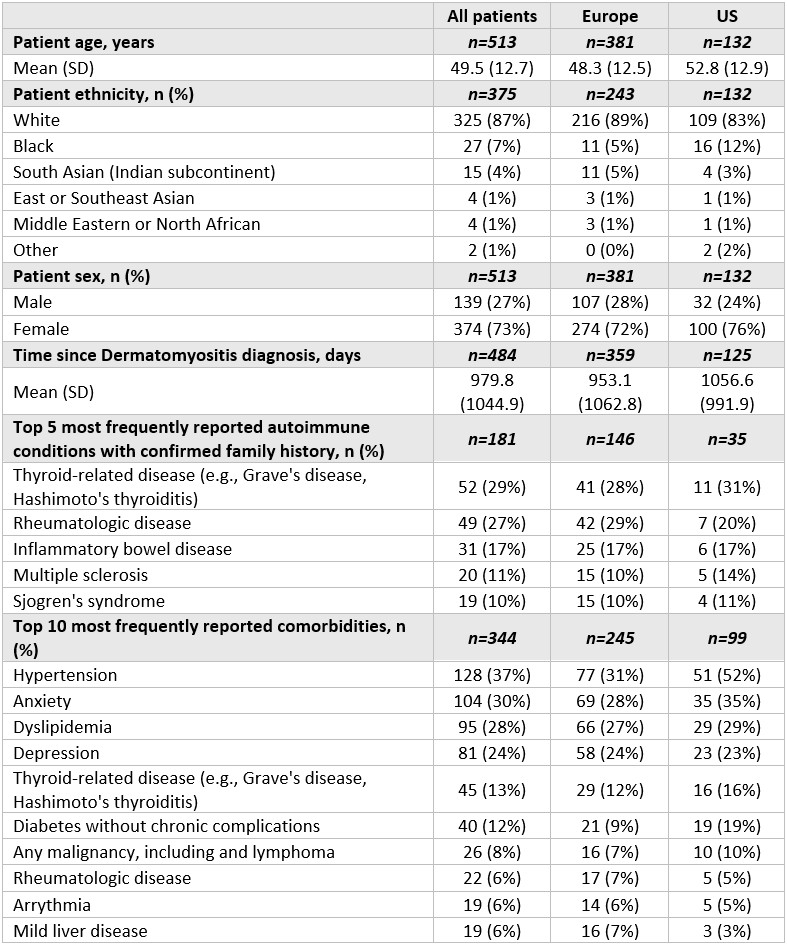 Table 1: Physician reported patient demographics at time of survey, across Europe and the United States
Table 1: Physician reported patient demographics at time of survey, across Europe and the United States
.jpg) Table 2: Diagnostic characteristics for dermatomyositis patients across Europe and the United States
Table 2: Diagnostic characteristics for dermatomyositis patients across Europe and the United States
.jpg) Figure 1: Proportion of patients who were initially diagnosed with a different condition, which was later identified as dermatomyositis, split by the first consulting physician type, across Europe and the United States
Figure 1: Proportion of patients who were initially diagnosed with a different condition, which was later identified as dermatomyositis, split by the first consulting physician type, across Europe and the United States
To cite this abstract in AMA style:
Yi E, Xenakis J, Blazos C, Garratt-Wheeldon J, Piercy J, Anderson P, Aggarwal R. Navigating Diagnostic Challenges: Insights into the Patient Journey and Delays in Diagnosing Dermatomyositis from a Real-world Survey in the United States and Europe [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/navigating-diagnostic-challenges-insights-into-the-patient-journey-and-delays-in-diagnosing-dermatomyositis-from-a-real-world-survey-in-the-united-states-and-europe/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/navigating-diagnostic-challenges-insights-into-the-patient-journey-and-delays-in-diagnosing-dermatomyositis-from-a-real-world-survey-in-the-united-states-and-europe/