Session Information
Date: Monday, October 27, 2025
Title: Abstracts: ARP I: Multidimensional Influences on Health in SLE (1686–1691)
Session Type: Abstract Session
Session Time: 4:15PM-4:30PM
Background/Purpose: Patients with childhood-onset systemic lupus erythematosus (cSLE) are at increased risk of low bone mineral density, with studies showing a 40% frequency of osteopenia (Lilleby, 2007). Guidelines for adults with SLE recommend yearly screening for patients on chronic steroids with dual X-ray absorptiometry (DXA). However, pediatric-specific protocols are lacking, leading to inconsistencies in care. The aim of this project was to assess current DXA screening practices at a pediatric rheumatology outpatient clinic and evaluate the early impact of a decision-tree algorithm on screening consistency.
Methods: A retrospective chart review of 70 cSLE patients seen from February 2024-May 2024 was performed to assess baseline screening practices and barriers. Quality improvement tools, including root cause analysis and a driver diagram with provider input, prompted the development of a decision-tree algorithm, based on current guidelines and expert input. This algorithm specified DXA eligibility (chronic steroids), frequency (yearly), and recommended sites (total body less head and lumbar spine). The algorithm was introduced to providers during an educational session in September 2024. DXA screening practices were then compared before and after the intervention.
Results: At baseline, screening rates varied by insurance status, with commercial insurance patients at 78.6%, government-insured at 66.7%, and uninsured at just 12.5%. Despite relatively high screening rates among the insured, 59.3% of eligible patients did not receive timely follow-up DXA scans and most DXA results were not accessible in the EMR. Additionally, there was significant inconsistency in anatomical site selection for DXA scans.
Following the educational intervention, chart review of 87 cSLE patients seen from January to April 2025 showed a marked improvement in correct anatomical site ordering, increasing from 0% to 52.6%. Appropriate, timely DXA ordering for patients due for follow up also increased from 40.7% to 100%. Overall, if a DXA was due, whether for an initial visit or follow-up visit, it was ordered 84% of the time, and the correct decision regarding DXA ordering was made 94.1% of the time. An informal, oral survey revealed ongoing difficulty among providers in instantly recalling the correct anatomical site, suggesting more sustainable interventions will help maintain consistent improvement.
Conclusion: These findings highlight a knowledge gap among providers of who, when, and where to DXA screen pediatric SLE patients. Early assessment of this intervention suggests a decision-tree algorithm can help address this gap by improving clarity, guiding providers to appropriate decisions, and standardizing DXA screening for optimal care. Ongoing efforts are focusing on sustainable implementation, including posting the algorithm in clinic workspaces and integrating a default DXA order set into the EMR, with future steps to address access disparities. Enhancing screening consistency may lead to earlier identification of bone density loss, enabling timely therapeutic adjustments and interventions to reduce fracture risk and long-term bone complications in this high-risk pediatric population.
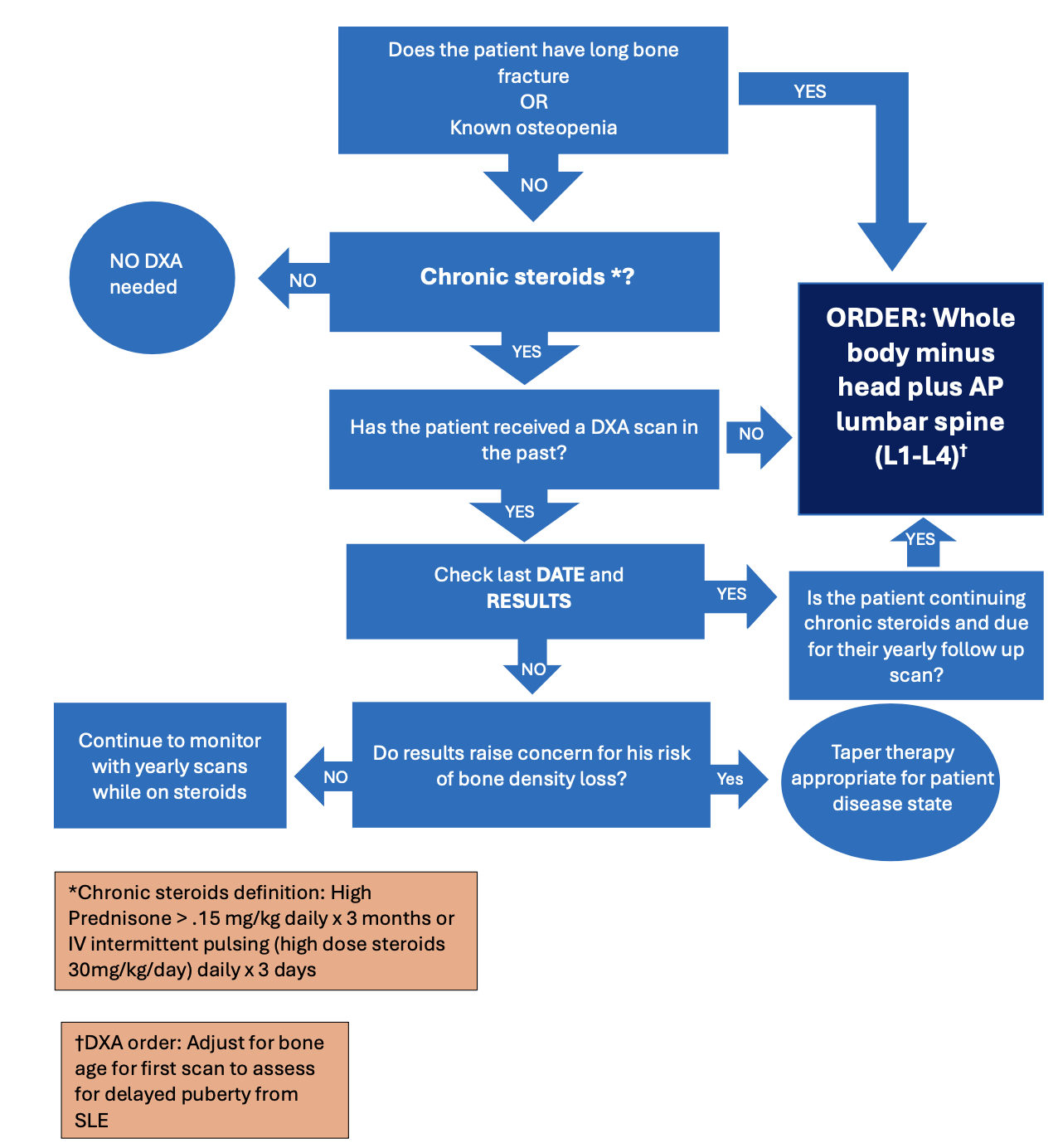 Decision-tree algorithm guiding DXA screening for childhood-onset SLE patients to standardize patient selection, timing, and site selection at a pediatric rheumatology outpatient clinic.
Decision-tree algorithm guiding DXA screening for childhood-onset SLE patients to standardize patient selection, timing, and site selection at a pediatric rheumatology outpatient clinic.
.jpg) Line chart illustrating improvements in timely follow-up DXA orders (40.7% to 100%) and correct anatomical site selection (0% to 52.6%) among pediatric SLE patients from baseline (January-May 2024) to post-intervention ((January-April 2025) after introduction of the DXA screening algorithm and guidelines in an education session.
Line chart illustrating improvements in timely follow-up DXA orders (40.7% to 100%) and correct anatomical site selection (0% to 52.6%) among pediatric SLE patients from baseline (January-May 2024) to post-intervention ((January-April 2025) after introduction of the DXA screening algorithm and guidelines in an education session.
.jpg) Pareto chart illustrating the frequency of anatomical sites ordered for DXA scans among pediatric SLE patients after introduction of the DXA screening algorithm and guidelines in an education session (January-April 2025), highlighting that 52.6% of provider orders adhered to recommended pediatric DXA guidelines.
Pareto chart illustrating the frequency of anatomical sites ordered for DXA scans among pediatric SLE patients after introduction of the DXA screening algorithm and guidelines in an education session (January-April 2025), highlighting that 52.6% of provider orders adhered to recommended pediatric DXA guidelines.
To cite this abstract in AMA style:
Gutierrez A, Armendariz S, Mogri M, Ciaglia K. Standardizing DXA Screening in Childhood-Onset Systemic Lupus Erythematosus at A Single Center: A Quality Improvement Initiative Using a Decision-Tree Algorithm [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/standardizing-dxa-screening-in-childhood-onset-systemic-lupus-erythematosus-at-a-single-center-a-quality-improvement-initiative-using-a-decision-tree-algorithm/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/standardizing-dxa-screening-in-childhood-onset-systemic-lupus-erythematosus-at-a-single-center-a-quality-improvement-initiative-using-a-decision-tree-algorithm/