Session Information
Session Type: Abstract Session
Session Time: 2:00PM-2:15PM
Background/Purpose: Childhood Sjögren Disease (cSjD) is a rare clinical phenotype lacking research on long-term outcomes and impact on the quality of life of young people (YP). This study aimed to characterise the natural history of cSjD into adulthood mapped onto the available classification criteria, the adult SjD clinical phenotypes (1) and the Florida Scoring System (FSS)-derived classification for cSjD (2).
Methods: Detailed patient and disease characteristics were collected retrospectively from a single centre, including assessment of disease activity, symptoms severity and damage using validated scores (ESSDAI, ESSPRI and SSDDI). Two paediatric diagnosis criteria, Bartunkova et al.,1999 (3) and Tomiita et al., 2019 (4), as well as the 2016 ACR/EULAR adult classification criteria (5) were tested at disease onset vs. last assessment.
Results: We identified 30 YP with cSjD (F:M=14:1, 60% White), aged 25.8+/-5.2 years, with symptoms onset at age 12.7+/- 3.3 years, follow-up 1-25 years (mean 10.5+/-5.4 years), and diagnosis delay of 3 weeks-5 years (Table). Manifestations at cSjD onset included: fatigue (73.3%), arthralgia (70%), dryness (56.6%), glandular swelling (33.6%), and skin rashes (30%). All 9 patients with >3 years diagnostic delay had dryness (100% vs. 38% of the ones diagnosed within 3 years, p< 0.001). All by one were ANA positive, while 83.3%, 40% and 43.3% were anti-Ro, anti-La and rheumatoid factor positive, respectively. All YP had ultrasound features of sialadenitis at diagnosis and 40% had salivary/lachrymal gland diagnostic biopsies. Three patients were diagnosed with lymphoma (10%), all within 3 years from diagnosis. All patients were treated with hydroxychloroquine, 19 with various cDMARDs, 7 with rituximab, one with belimumab and 3 with cyclophosphamide. At the last assessment, the median ESSDAI was 2 (IQR 2-8), median ESSPRI was 5.33 (IQR 3-7); 17 (56.6%) cSjD patients had damage due to decreased saliva/tear secretion, and 3 (10%) experienced teeth loss. At the time of diagnosis compared to last assessment, 12(40%) vs. 20(66.6%) fulfilled the ACR/EULAR criteria, 9(29%) vs. 14(46.6%) fulfilled the paediatric Bartunkova criteria and 12(40%) vs. 19(61.2%) had at least a ‘probable’ diagnosis of cSjD based on Tomiita criteria. At the last assessment, 36.6% had 'high' vs. 30% 'low symptoms burden', while 26.6% had 'dominant pain' and 6.66% 'dominant dryness with fatigue' symptoms. At presentation, 56.6% patients could not be mapped onto any of the FSS-derived clusters as they presented with either 'high' or 'low symptoms and positive tests', reflecting their longer diagnosis delay compared to the cSjD cohort used for the FSS classification.
Conclusion: This unique longitudinal cohort analysis revealed differences between cSjD and adult SjD clinical phenotypes, and poor performance of the FSS for cSjD classification at presentation. Almost 2/3 patients could not be initially classified/diagnosed by any of the available criteria, and 1/3 still could not be classified even after 10 years of follow-up. These findings highlight the critical need for adequate classification/research in cSjD, characterised by early damage accrual and 10% risk of lymphoma in this unique adult cohort.
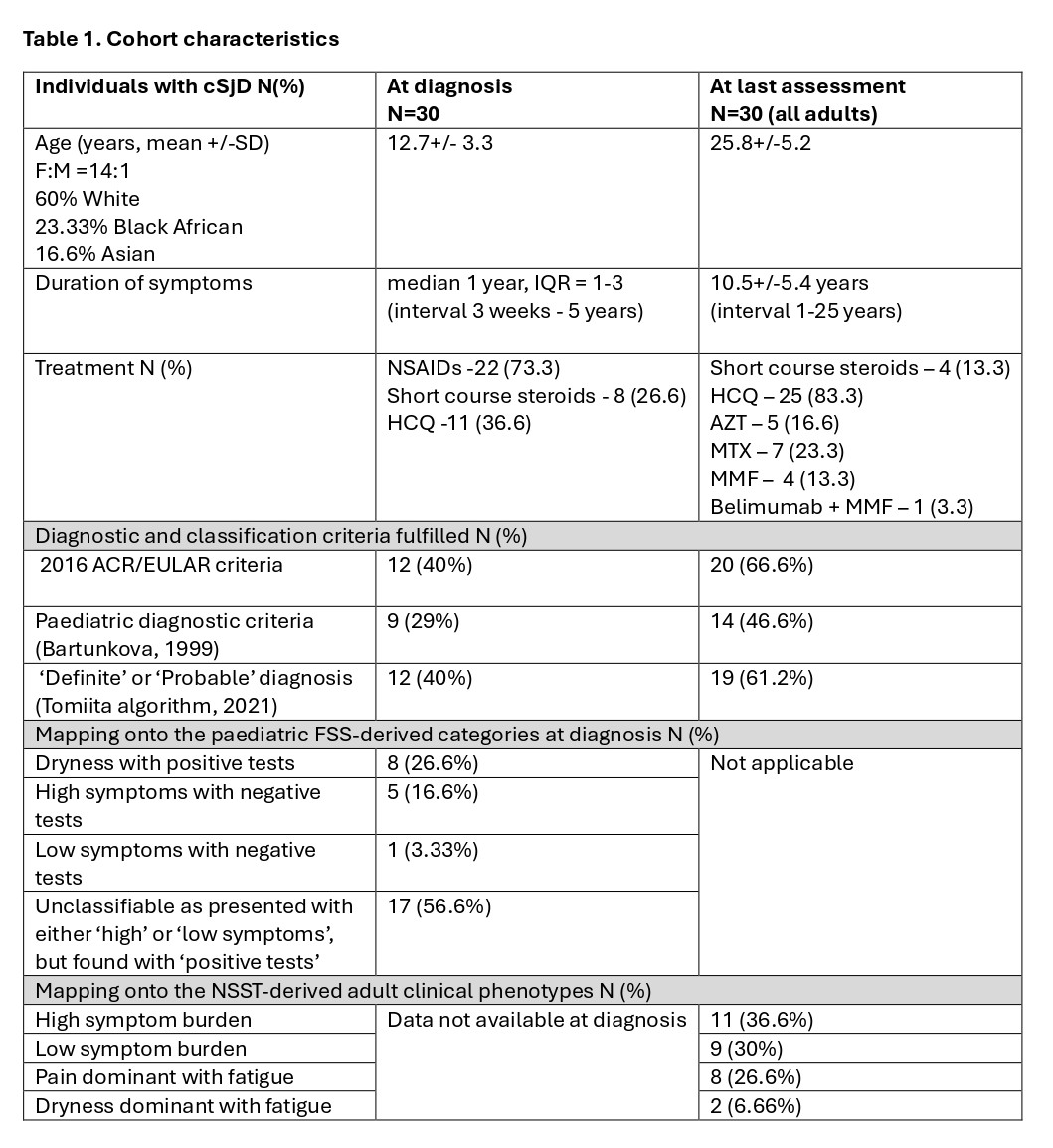 Legend: ACR – American College of Rheumatology; AZT – azathioprine; cSjD – Childhood onset Sjögren Disease; EULAR – European Alliance of Associations for Rheumatology; F – females; FSS – Florida Scoring System; H – hydroxychloroquine; M – males; MMF – mycophenolate mofetil; MTX – methotrexate; N – number; NSST – Newcastle Sjögren Stratification Tool.
Legend: ACR – American College of Rheumatology; AZT – azathioprine; cSjD – Childhood onset Sjögren Disease; EULAR – European Alliance of Associations for Rheumatology; F – females; FSS – Florida Scoring System; H – hydroxychloroquine; M – males; MMF – mycophenolate mofetil; MTX – methotrexate; N – number; NSST – Newcastle Sjögren Stratification Tool.
To cite this abstract in AMA style:
Ciurtin C, Gotch R, Peckham H, Wilson R, AlObaidi M, C Jury E. Classification criteria, disease phenotypes and long-term outcomes of childhood Sjögren’s Disease into adulthood [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/classification-criteria-disease-phenotypes-and-long-term-outcomes-of-childhood-sjogrens-disease-into-adulthood/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/classification-criteria-disease-phenotypes-and-long-term-outcomes-of-childhood-sjogrens-disease-into-adulthood/