Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Prior studies have observed that patient-reported outcomes, such as pain, are risk factors for progression to difficult-to-treat RA (D2T-RA), a state of multi-treatment failure. However, the impact of longitudinal trajectories in pain on the risk of D2T-RA is not known.
Methods: We used data from the longitudinal Brigham and Women’s Hospital Rheumatoid Arthritis Sequential Study (BRASS) registry. Study participants included those who were not classified as having D2T-RA at baseline and had at least two assessments of pain on the MDHAQ pain scale questionnaire. D2T-RA was defined using EULAR 2021 criteria and follow-up continued through earliest of either qualifying for D2T-RA or the last study visit. We modeled trajectories of pain using latent class mixed models in R, and evaluated random intercepts and/or slopes, link functions (linear, beta, quadratic splines), and 0-4 latent classes. We used BIC, entropy, and class membership to select the best fitting model. We evaluated the hazard of progressing to D2T-RA in extended Cox Proportional hazards models. Three sets of models were assessed, including pain measures only at baseline, the current pain level, and the pain trajectory. All models were adjusted for age and gender.
Results: Our analyses included 1,458 (92% of 1,581 BRASS enrollees) with mean age of 56 years, 82% female, and 20% with early RA. Over a mean follow-up of 81 months, 196 (13%) developed D2T-RA. We identified three latent classes of pain trajectories during follow-up, described as moderate-increasing (42%), low-stable (47%), and low-resolving (11%) (Figure 1). Among patients who progressed to D2T-RA during follow-up, 68% followed a moderate-increasing pain trajectory; 31% a low-stable trajectory, and < 1% a low-improving trajectory. In contrast, among those who did not progress to D2T-RA, the distribution was 38% moderate-increasing, 49% low-stable, and 13% low-improving. In age and sex adjusted extended Cox proportional hazards models (Table 1) we observed that a five unit increase in baseline pain or current observed pain was associated with 8-12% increased hazards of progression to D2T-RA (HR=1.08 & 1.12), respectively. In a model that included predicted pain (per five-unit increase) based on latent classes we observed 24% increased hazards of D2T-RA (HR=1.24). Finally, in a model including pain trajectory categories, we observed a 3.1-fold increased hazards of D2T-RA for participants with a moderate-increasing pain trajectory and a 93% reduction in hazards (HR =0.07) for participants with a low-resolving pain trajectory, compared to participants with a low-stable trajectory.
Conclusion: In this cohort of patients at risk of progression to D2T-RA, pain trajectories were stronger predictors than baseline, or current pain levels. Future research should explore joint trajectory models to better account for uncertainty.
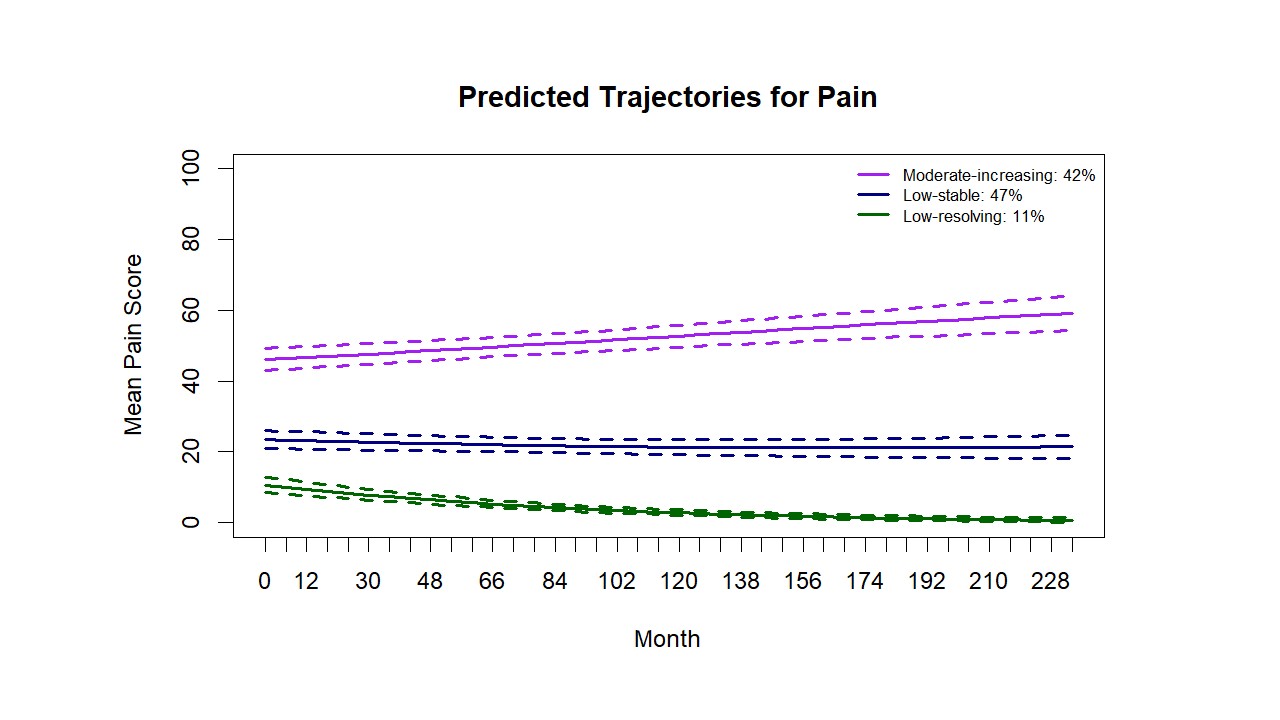 Figure 1. Latent Classes of Pain Trajectories in Participants with RA
Figure 1. Latent Classes of Pain Trajectories in Participants with RA
.jpg) Table 1. Extended Cox Proportional Hazards for Progression to D2T-RA
Table 1. Extended Cox Proportional Hazards for Progression to D2T-RA
To cite this abstract in AMA style:
Paudel M, Santacroce L, Shadick N, Weinblatt M, Solomon D. Longitudinal Trajectory Models to Assess Pain and Risk of Difficult-to-Treat Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/longitudinal-trajectory-models-to-assess-pain-and-risk-of-difficult-to-treat-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/longitudinal-trajectory-models-to-assess-pain-and-risk-of-difficult-to-treat-rheumatoid-arthritis/