Session Information
Date: Monday, October 27, 2025
Title: (1553–1591) Systemic Sclerosis & Related Disorders – Clinical Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: The clinical course of interstitial lung disease (ILD) in systemic sclerosis (SSc) is highly variable–some patients experience progressive loss of lung function while others remain stable. Although risk factors such as early disease, diffuse cutaneous subtype, Black race, and >20% ILD on baseline CT increase the likelihood of progression, ILD progression can also occur in their absence. This study aimed to develop radiomic profiles linked to pulmonary function decline by analyzing quantitative CT measures of lung parenchymal and vascular abnormalities in early SSc.
Methods: A retrospective cohort of adult (≥18 yrs) patients with systemic sclerosis (SSc) seen at an academic center (1/1/2007–12/31/2018) was identified using ICD-9/10 codes. Records were reviewed, and patients included if they met ACR/EULAR 2013 SSc classification criteria or ≥3/5 CREST criteria and had ILD. Inclusion required a baseline high-resolution CT (HRCT) ±2 yrs of SSc diagnosis and a PFT ±6 mo. of HRCT. Patients with infection, pleural effusion, cardiogenic edema, or non-SSc ILD were excluded. CALIPER software quantified six lung features (normal, ground glass opacities (GGO), reticular densities (RD), honeycombing (HC), hyperlucency, and pulmonary vascular related structures (PVRS)) by lung zone (upper/middle/lower, central/peripheral). Each feature was expressed as a % of lung volume for that zone. Percent predicted forced vital capacity (ppFVC) was standardized using the GLI 2022 equations.1 Latent Profile Analysis (LPA) identified radiomic clusters from CALIPER measurements. Mixed effects models estimated annual ppFVC decline by cluster, adjusting for baseline ppFVC, including linear and quadratic effects for the change over time.
Results: Of 1,399 SSc patients identified, 712 had ILD, 315 had a CT ±2 yrs of SSc diagnosis, and 116 met inclusion criteria with ≥1 follow-up PFT. LPA identified two radiomic profiles (LP1 & LP2). LP1 had lower percentages of ILD, GGO, RD, HC, and PVRS (Table 1). There were no significant differences in demographics, smoking history, SSc dx. dur., subtype or other clinical features, anti-Scl70, or anti-centromere Abs (Table 1). RNA Pol III was less frequent in LP1 than LP2 (18% vs. 46%, p=0.048). LP1 had a shorter interval from ILD dx. to HRCT (median 0.0 vs. 0.5 yrs; p< 0.001), and better lung function at baseline (median ppFVC (85% vs. 75%) and ppDLCO (64% vs. 49%), both p< 0.001). In longitudinal analysis, LP2 had a faster rate of ppFVC decline: -2.66% per year (95% CI: –4.65 to –0.67; p=0.011) relative to LP1, adjusting for baseline ppFVC (Table 2, Model 1). This association was slightly attenuated after adjusting for age, sex, ILD dur., Scl-70(+), and diffuse subtype (–2.18% per year; 95% CI: –4.35 to 0.01; p=0.054; Table 2, Model 2; Fig 1).
Conclusion: Two early SSc-ILD radiomic phenotypes were identified. Frequencies of clinical risk factors for ILD progression were similar between profiles. One radiomic profile was associated with greater parenchymal and vascular abnormalities and faster lung function decline. Imaging-based phenotyping using radiomic biomarkers may enhance risk stratification and identify patients at higher risk for ILD progression. Ref. 1. Bowerman, C. et. Al., AJRCCM, 2022.
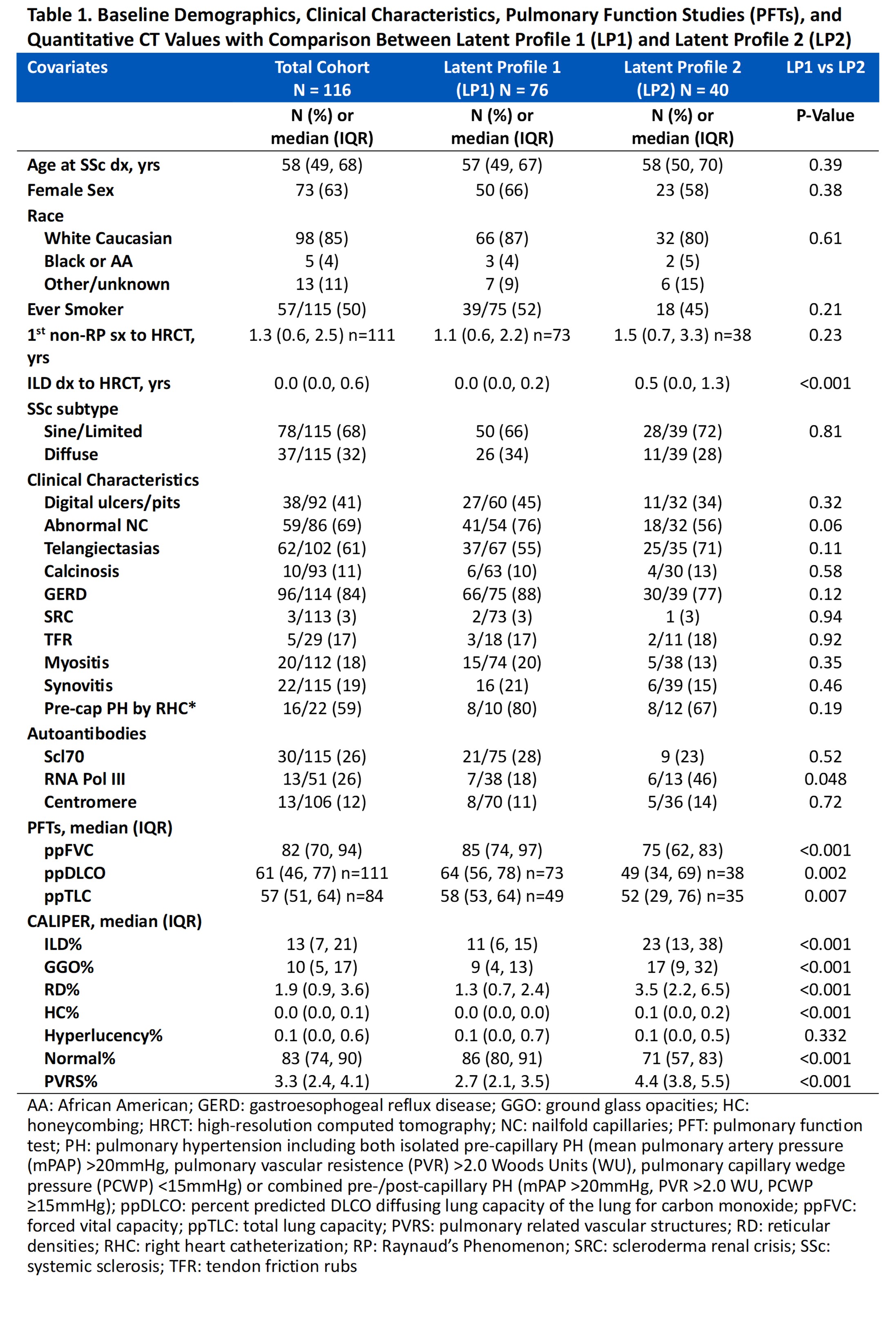 Table 1. Baseline Demographics, Clinical Characteristics, Pulmonary Function Studies (PFTs), and Quantitative CT Values with Comparison Between Latent Profile 1 (LP1) and Latent Profile 2 (LP2)
Table 1. Baseline Demographics, Clinical Characteristics, Pulmonary Function Studies (PFTs), and Quantitative CT Values with Comparison Between Latent Profile 1 (LP1) and Latent Profile 2 (LP2)
.jpg) Table 2. Estimated Difference in the Change in ppFVC per year for Latent Profile 2 Compared to Latent Profile 1
Table 2. Estimated Difference in the Change in ppFVC per year for Latent Profile 2 Compared to Latent Profile 1
.jpg) Figure 1. Difference in the Estimated Rate of Decline in percent predicted FVC (ppFVC) per year for Latent Profile (LP) 1 vs. LP 2, adjusting for age, sex, baseline ppFVC, ILD duration, diffuse cutaneous disease, and a positive Scl70
Figure 1. Difference in the Estimated Rate of Decline in percent predicted FVC (ppFVC) per year for Latent Profile (LP) 1 vs. LP 2, adjusting for age, sex, baseline ppFVC, ILD duration, diffuse cutaneous disease, and a positive Scl70
To cite this abstract in AMA style:
Hinze A, Katurkuri N, Vassallo R, Shah A, Lennon R, Bartholmai B, Crowson C. Latent Profiles of Parenchymal Abnormalities and Vascular Features Measured by Quantitative CT Identifies a Subgroup of Systemic Sclerosis Patients With a Greater Lung Function Decline Over Time [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/latent-profiles-of-parenchymal-abnormalities-and-vascular-features-measured-by-quantitative-ct-identifies-a-subgroup-of-systemic-sclerosis-patients-with-a-greater-lung-function-decline-over-time/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/latent-profiles-of-parenchymal-abnormalities-and-vascular-features-measured-by-quantitative-ct-identifies-a-subgroup-of-systemic-sclerosis-patients-with-a-greater-lung-function-decline-over-time/