Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: The 2023 EULAR recommendations for the management of Rheumatoid Arthritis (RA) emphasizes theimportance of limiting the dose and duration of glucocorticoids (GC) used in early disease. However, norecommendation about the preferred route of GC administration is available, nor is it known if GC route isassociated with total GC exposure. In this study we describe the route of GC administration in patients with early RA (ERA), and determine if GC route is associated with the likelihood of being GC-free and/or requiring advanced therapy at 12 months.
Methods: Participants included newly diagnosed RA patients (symptoms < 1 year) enrolled in the Canadian Early ArthritisCohort (CATCH) between (dates) and excluded if they reported GC use 90 days prior to baseline, were onadvanced therapy by 3 months, or had < 12 months. Patients were stratified by use of GC during the first 3months of follow-up: none; oral only; parenteral only (intramuscular or intraarticular); or both (oral+parenteral). Multivariate logistic regression adjusted by confounders was used to calculate the OR of GC useat 6 and 12 months and/or progression to advanced therapies (biologics or JAKi).
Results: The sample included 2,222 ERA patients. Mean (SD) age was 55 (15), disease duration 5.5 (3) months, 73%were female, and 86% were white, 69% were initially on methotrexate (MTX) at a mean dose of 20.1 (4.2)mg/week. Mean CDAI at baseline and 12-month scores were 26 (14) and 7.5 (8.6).The majority (1,661; 75%) received no GC; oral-only GC was 421 (19%); parenteral-only GC was 121 (5%), andboth oral and parenteral was 19 (1%). Mean CDAI at baseline was lowest in the no GC and highest in thosereceiving both (24.1 vs 31.6, vs 30.2, vs 32.8, p < 0.0001), but no differences were observed among groups at 12months. GC and advanced therapeutics at 12 months were: 8% and 7% (no GC); 47% and 14% (oral); 26% and14% (parenteral); 63% and 16% (both). Table 1 shows that any GC use, particularly oral-only, increases odds ofchronic GC use at 6 and 12 months, as well as advanced therapy utilization. Figure 1 features a Sankey diagramillustrating changes in GC use over 12 months.
Conclusion: Initial use of GC is low despite EULAR recommendations suggesting their use for patients with higher baselinedisease activity. Among patients with active early RA, those receiving parenteral GC were half as likely toremain on GC at 12 months, compared to those using oral GC. Both GC groups had similar rates of use ofadvanced treatment use, which were higher compared to the no GC group. Parenteral GC use may supportearlier discontinuation of steroids.
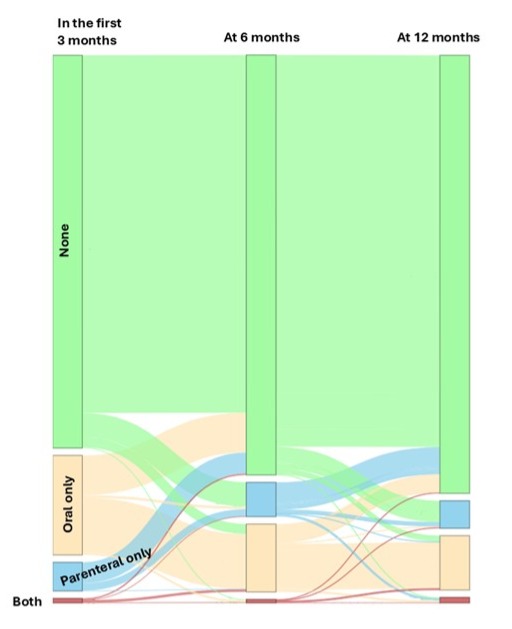 Table 1. Multivariate logistic regression estimating the odds for GC and advanced therapy use over time
Table 1. Multivariate logistic regression estimating the odds for GC and advanced therapy use over time
To cite this abstract in AMA style:
Fernandez Codina A, Valois M, Bartlett S, Wahed M, Allard-Chamard H, Bessette L, Hazlewood G, Hitchon C, Kuriya B, Bykerk V, Pope J. Use of parenteral compared to oral glucocorticoids in early rheumatoid arthritis is superior for chance ofbeing off steroids and escalation of therapy at 1 year [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/use-of-parenteral-compared-to-oral-glucocorticoids-in-early-rheumatoid-arthritis-is-superior-for-chance-ofbeing-off-steroids-and-escalation-of-therapy-at-1-year/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/use-of-parenteral-compared-to-oral-glucocorticoids-in-early-rheumatoid-arthritis-is-superior-for-chance-ofbeing-off-steroids-and-escalation-of-therapy-at-1-year/