Session Information
Date: Monday, October 27, 2025
Title: (1191–1220) Muscle Biology, Myositis & Myopathies – Basic & Clinical Science Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Anti-Ro52 antibodies are commonly detected in idiopathic inflammatory myopathies (IIMs), yet their clinical significance remains incompletely defined. There is evidence that it coexists with anti-synthetase antibodies (ARS). We aimed to investigate the phenotype, survival and antibody coexistence of anti-Ro52 patients within a IIM cohort.
Methods: Retrospective analysis with clinical information regarding skin (CDASI score, typical signs), muscle (MMT-8 score, CPK levels), lung involvement (CT thorax pattern and % predicted Forced Vital Capacity), dysphagia and survival in months, laboratory test (ferritin, LDH, WBC, Hb) and autoantibody profile was performed. Antibody test for Myositis Specific Autoantibodies (MSA) and Myositis Associated Autoantibodies (MAA) was done with myo blot and ANA with indirect immunofluorescence.
Results: A total of 107 patients were analyzed, including 28 (26.2%) positives for anti-Ro52. Anti-Ro52 positivity was significantly associated with antisynthetase syndrome (AS) (p = 0.009), with post hoc analysis revealing that AS patients were disproportionately represented among Ro52-positive individuals (standardized residual +2.5). Antibody coexistence was significant for anti-Jo1 (p=0.001) and anti-FARS (p< 0.001).Patients with anti-Ro52 antibodies were diagnosed at a younger age (mean= 55.6 SD ± 12.36 vs. 61.4 years SD ±12.52, p = 0.039) and exhibited significantly lower FVC% at diagnosis (mean=72.1% SD ± 22.21 vs. 88.3% SD ±14.56, p = 0.001). Lung involvement was significantly more frequent in Ro52-positive patients (64.3% vs. 35.4%, p = 0.015), and CT thorax patterns differed by antibody status (p = 0.015), with non-specific interstitial pneumonia (NSIP) more prevalent among Ro52-positive patients (standardized residual +2.1). While overall survival was lower in the Ro52-positive group, the difference was not statistically significant (p=0.39).No significant differences were observed in malignancy rates, skin involvement (CDASI score and main typical skin signs), muscle involvement (MMT-8 score, CPK levels) . No difference was seen in main commorbidities including Hypertension, diabetes, coronary artery disease, hypothyroidism and osteoporosis (p=ns). Anti-Ro52-(+) patients did not differ in performance status. Although there was a trend towards more severe scores (PS3 or 4)p=0.09.
Conclusion: These findings highlight a potential role of anti-Ro52 as a marker of severe, lung-predominant IIM phenotype but they do not support any other distinct clinical and radiographic profile associated with anti-Ro52 antibodies.
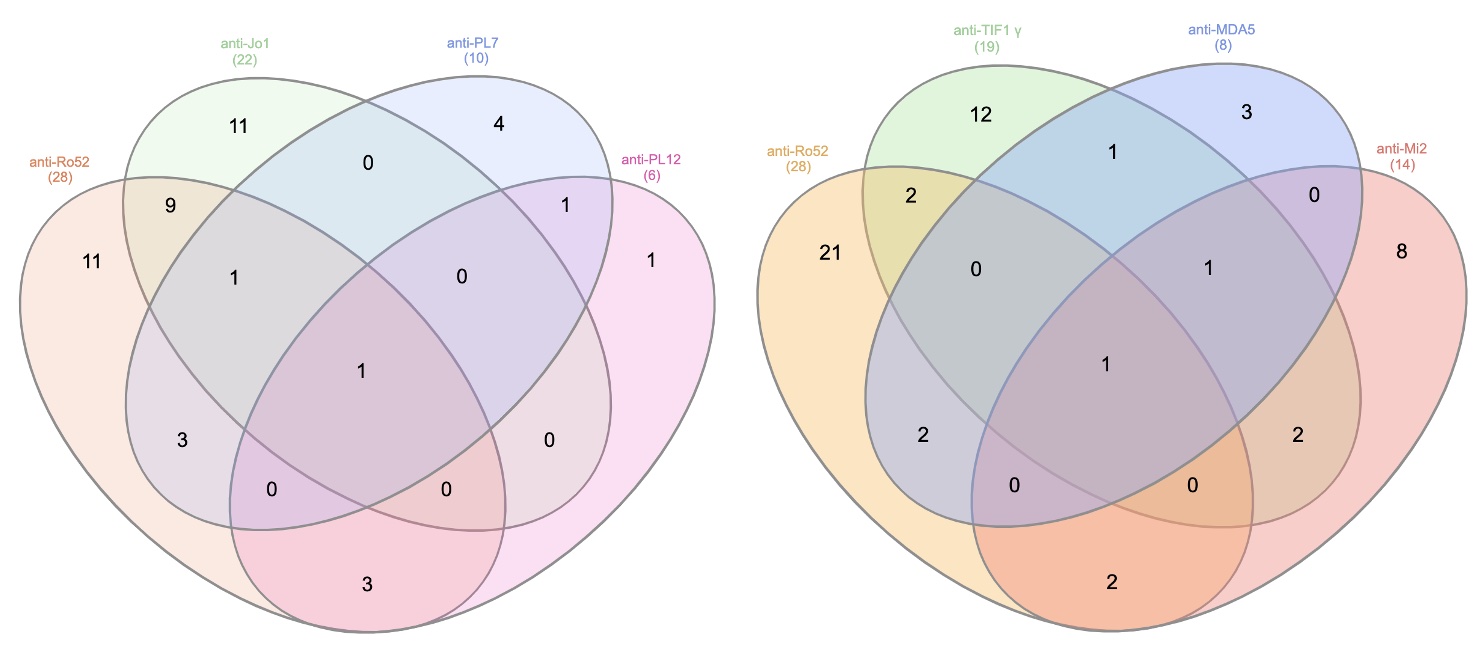 Venn diagramms depicting coexistence of anti-Ro-52 with with most common MAA (anti-Jo1, anti-PL7, anti-PL12)on the left and most common MSA (anti-TIF1γ, anti-Mi2, anti-MDA5) on the right in our cohort.
Venn diagramms depicting coexistence of anti-Ro-52 with with most common MAA (anti-Jo1, anti-PL7, anti-PL12)on the left and most common MSA (anti-TIF1γ, anti-Mi2, anti-MDA5) on the right in our cohort.
.jpg) Disease subtypes distribution across our cohort. Blue box represents anti-Ro52(-) while orange box anti-Ro52(+) cases
Disease subtypes distribution across our cohort. Blue box represents anti-Ro52(-) while orange box anti-Ro52(+) cases
.jpg) Bar chart with coexistence of percentage of anti-Ro52 (+) with other autoantibodies
Bar chart with coexistence of percentage of anti-Ro52 (+) with other autoantibodies
To cite this abstract in AMA style:
Syrmou V, Alexiou I, Liaskos C, Patrikiou E, SIMOPOULOU T, Katsiari C, Bogdanos D. Anti-Ro52 Antibody Identifies Patients with More Severe Lung disease among Patients with Idiopathic Inflammatory Myopathy [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/anti-ro52-antibody-identifies-patients-with-more-severe-lung-disease-among-patients-with-idiopathic-inflammatory-myopathy/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/anti-ro52-antibody-identifies-patients-with-more-severe-lung-disease-among-patients-with-idiopathic-inflammatory-myopathy/