Session Information
Date: Monday, October 27, 2025
Title: (1191–1220) Muscle Biology, Myositis & Myopathies – Basic & Clinical Science Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Interstitial lung disease (ILD) is a common and severe complication of idiopathic inflammatory myopathies (IIM), adversely impacting clinical outcomes. While the ACR/CHEST guideline recommends ILD screening in IIM patients with specific risk factors (Table 1), validation of these predictors in diverse populations remains limited. This study evaluated the utility of ACR/CHEST risk factors for ILD development in a Hong Kong IIM cohort (MyoHK).
Methods: MyoHK was a multicentre observational cohort that collected longitudinal data from IIM patients from 7 rheumatology centers in Hong Kong. IIM patients with at least 6 months of follow-up data were analyzed after excluding patients with unknown myositis-specific or myositis-associated antibodies (MSA/MAA). Data was reviewed from Jan 2024 to Feb 2025. Demographic, clinical, and serological data at IIM diagnosis were recorded. ILD was confirmed by compatible CT thorax findings or histology. The time between IIM and ILD diagnosis was determined. Multivariable regression was performed to identify the independent predictors of ILD.
Results: A total of 665 patients were analyzed and 503 (75.6%) had at least one clinical or serological risk factor for developing ILD at IIM diagnosis. More than half (53.7%) of IIM patients had ILD and 28.6% had no respiratory symptoms including cough, dyspnoea, or Velcro crackles at onset (Figure 1). There were more female patients in the IIM-ILD group (73.3% vs 63.6%, p=0.007) but there was no difference between mean age at diagnosis (55.6 ± 12.5 vs 56.7 ± 15.8, p=0.35) and median follow-up duration (73 (interquartile range: 27 – 130.5) vs 54 (27 – 131) months, p=0.651). Over 60% of ILD were diagnosed within 6 months of IIM diagnosis but ILD preceded IIM diagnosis in 62 (17.4%) patients.Arthritis (57.7% vs 21.8%, p < 0.001), ulcerative lesions (12.9% vs 1.6%, p < 0.001), and mechanic’s hands (25.2% vs 4.9%, p < 0.001) were more common in IIM-ILD group (Table 2). Regarding MSA/MAA status, antibodies against MDA5 (28.0% vs 2.9%, p < 0.001), Jo1 (23.8% vs 2.9%), PL7 (11.2% vs 5.2%, p=0.005), EJ (7.3% vs 1.3%, p < 0.001) and Ro52 (62.7% vs 28.9%, p < 0.001) were more frequently identified among ILD patients. Independent risk factors for ILD development in line with the ACR/CHEST guideline included anti-MDA5 positivity (Odds ratio (OR):12.3, 95% CI: 4.8 - 31.0), anti-Jo1 positivity (OR: 6.8, 95% CI: 2.7 – 12.2), anti-EJ positivity (OR: 5.7, 95% CI: 1.37 – 23.6), anti-Ro52 positivity (OR: 2.8, 95% CI: 1.7 – 4.6), mechanic’s hands (OR: 2.5, 95% CI: 1.1 – 5.7) and arthritis (OR: 1.8, 95%CI:1.1 – 3.2). Fever (OR: 2.27, 95% CI = 1.5 – 4.9) and Raynaud’s phenomenon (OR: 2.1, 95%CI: 1.0 – 4.4) were identified as additional risk factors for ILD development. Only 5.3% of ILD patients lacked guideline-recommended risk factors.
Conclusion: The study validated the risk factors from ACR/CHEST guidelines in IIM patients in Hong Kong. However, the absence of respiratory symptoms or guideline-specified risk factors could not exclude the possibility of ILD, underscoring the need for clinical vigilance.
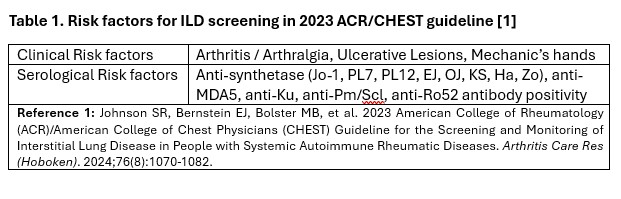 Risk factors for ILD screening in 2023 ACR/CHEST guideline
Risk factors for ILD screening in 2023 ACR/CHEST guideline
.jpg) Table 2. Baseline Characteristics of IIM patients
Table 2. Baseline Characteristics of IIM patients
.jpg) Figure 1. Distribution of clinical and serological risk factors and occurrence of ILD among IIM patients
Figure 1. Distribution of clinical and serological risk factors and occurrence of ILD among IIM patients
To cite this abstract in AMA style:
Yam K, Luk L, Lao W, Chan C, Chan D, Lai B, Ho R, Tang V, So H, Tang I. High Prevalence of Asymptomatic Interstitial Lung Disease in Idiopathic Inflammatory Myopathies: Validation of ACR/CHEST Risk Factors in a Hong Kong Cohort [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/high-prevalence-of-asymptomatic-interstitial-lung-disease-in-idiopathic-inflammatory-myopathies-validation-of-acr-chest-risk-factors-in-a-hong-kong-cohort/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/high-prevalence-of-asymptomatic-interstitial-lung-disease-in-idiopathic-inflammatory-myopathies-validation-of-acr-chest-risk-factors-in-a-hong-kong-cohort/