Session Information
Date: Monday, October 27, 2025
Title: (1147–1190) Miscellaneous Rheumatic & Inflammatory Diseases Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: The novel diagnosis of VEXAS in 2020 led to the proposed possibility of a new category of hematoinflammatory syndromes linking clinically overlapping hematologic and autoinflammatory diseases with multiorgan involvement, laboratory and histopathologic features, and genetic mutation in parallel to the clinical picture of VEXAS syndrome and hemophagocytosis (HLH/MAS)1, 2. Lack of definition and standard of care diagnostic and treatment algorithms for this subset of diagnoses pose critical complexities and challenges, given their high morbidity and mortality, hence the need for understanding these disease entities to improve patient outcomes. This study aims to review baseline disease characteristics, diagnostic and treatment approaches, and outcomes at our academic center.
Methods: This is IRB-approved retrospective analysis on all patients 18-89 years old with hematoinflammatory manifestations at University of Florida between 01/01/2020 to 03/31/2025. IDR analysis obtained 162 patients with ICD-10-specific codes for HLH/MAS/VEXAS (D76.1,.3,.2;M04.1,.2,.8,.9) for individual chart review. Inclusion criteria were determined by clinicians’ discretion for diagnosis based on HLH 2004/MAS 2016 criteria, histopathology, and/or genetic tests. Subsequent data was collected and analyzed.
Results: Baseline characteristics are summarized (Table 1), with 23 patients meeting criteria for hematoinflammatory diagnosis. Mean age at diagnosis was 40 years. Mean duration of symptoms was 16.35 weeks before diagnosis. Majority were Caucasian(43%), male(57%), and younger age of < 50 years (61%). Most common underlying diagnoses are autoimmune diseases(48%), infection (30%), primarily Epstein-Barr virus (EBV), followed by hematologic etiologies (17%). Constitutional symptoms, such as fever and fatigue, and hematologic findings were present in all patients (Figure 1); gastrointestinal, lymphadenopathy, and dermatologic symptoms in 40%; 91% had at least 3 organ systems involved upon initial presentation. Diagnoses were mainly HLH (48%) and MAS (35%) with fever, elevated ferritin (mean,14,186ng/ml), and cytopenias as most common presentation. Biopsy(78%) and genetic testing (43%)revealed 7 with positive vacuoles and hemophagocytes; 1 with MDS diagnosed with VEXAS after genetic confirmation, and only revealed vacuoles with repeat biopsy after 3 months. Previous treatments comprised majority with csDMARDs.Figure 2 outlines the treatments received following diagnosis-glucocorticoid (100%), Anakinra (43%), and Etoposide (26%). Mean length of stay before discharge was 4 weeks;3 patients died due to infections and hospital complications.
Conclusion: This study provides a heterogeneous presentation of hematoinflammatory syndromes at our center. Due to diagnostic complexities and multiorgan manifestations, clinicians must be cognizant of their broader definitions, familiarize with their most frequent diagnostic associations, and monitor disease indicators (e.g., serial serum ferritin levels, biopsy, etc), if with high clinical suspicion. This leads to earlier recognition and more optimal therapeutic strategies for hematoinflammatory syndromes to improve clinical outcomes.
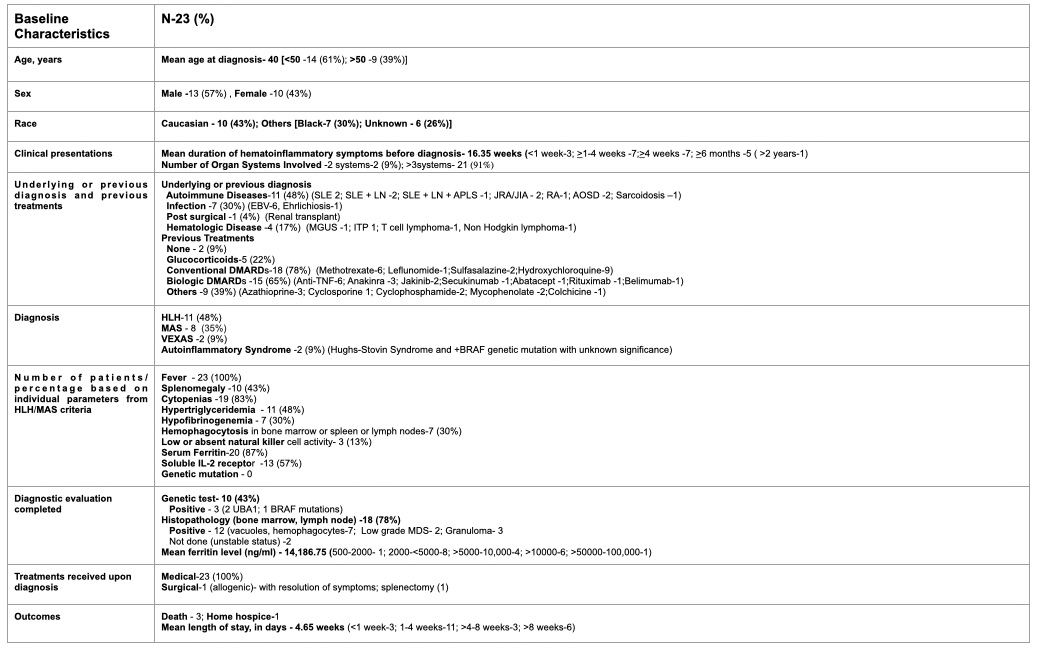 Table 1. Baseline characteristics of the study population. SLE, Systemic Lupus Erythematosus; LN, Lupus Nephritis; APLS, Antiphospholipid Antibody Syndrome; AOSD, Adult Onset Still’s Disease; EBV, Epstein-Barr virus; MGUS, Monoclonal Gammopathy of Undetermined Significance; ITP, Idiopathic Thrombocytopenic Purpura; DMARDs, Disease-modifying antirheumatic drugs; TNF, Tumor Necrosis Factor; HLH, Hemophagocytic lymphohistiocytosis; MAS, Macrophage activation syndrome; VEXAS syndrome (vacuoles, E1 enzyme, X-linked, autoinflammatory, somatic); MDS, Myelodysplastic syndrome.
Table 1. Baseline characteristics of the study population. SLE, Systemic Lupus Erythematosus; LN, Lupus Nephritis; APLS, Antiphospholipid Antibody Syndrome; AOSD, Adult Onset Still’s Disease; EBV, Epstein-Barr virus; MGUS, Monoclonal Gammopathy of Undetermined Significance; ITP, Idiopathic Thrombocytopenic Purpura; DMARDs, Disease-modifying antirheumatic drugs; TNF, Tumor Necrosis Factor; HLH, Hemophagocytic lymphohistiocytosis; MAS, Macrophage activation syndrome; VEXAS syndrome (vacuoles, E1 enzyme, X-linked, autoinflammatory, somatic); MDS, Myelodysplastic syndrome.
.jpg) Figure 1. Frequencies of system-based organ manifestations present in our patients with hematoinflammatory syndromes.
Figure 1. Frequencies of system-based organ manifestations present in our patients with hematoinflammatory syndromes.
.jpg) Figure 2. Treatment received with the corresponding number of patients and prevailing treatment approaches over the past 5 Years following hematoinflammatory diagnosis.
Figure 2. Treatment received with the corresponding number of patients and prevailing treatment approaches over the past 5 Years following hematoinflammatory diagnosis.
To cite this abstract in AMA style:
Kuzhuppilly Arcilla C, Kirsch G, Cargill M, Kaeley G. New Disease Classification in the Block? A 5-year Retrospective Review on Clinical Profiles and Mortality Outcomes of Patients Presenting with Hematoinflammatory Syndromes at a University Center in Florida [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/new-disease-classification-in-the-block-a-5-year-retrospective-review-on-clinical-profiles-and-mortality-outcomes-of-patients-presenting-with-hematoinflammatory-syndromes-at-a-university-center-in-f/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/new-disease-classification-in-the-block-a-5-year-retrospective-review-on-clinical-profiles-and-mortality-outcomes-of-patients-presenting-with-hematoinflammatory-syndromes-at-a-university-center-in-f/