Session Information
Date: Sunday, October 26, 2025
Title: (0765–0771) Orthopedics, Low Back Pain, & Rehabilitation Poster
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Knee osteoarthritis (OA) is a chronic disease with no current cure and a leading cause of disability among adults. Treatment for knee OA focuses on symptom management, with physical activity (PA) and Corticosteroid (CS) injections being strongly recommended. However, increased utilization of CS injections may increase the risk of total joint replacement, and those with higher Kellgren-Lawrence (KL) grades have been shown to have higher odds of receiving a CS injection. Further, it is unknown if PA mitigates the use of CS injections for those with worse radiographic evidence of knee OA. The purpose of this study was to determine if PA modifies the relationship between radiographic OA (ROA) presence and utilization of CS injections during a 5-year follow-up period in adults with or at high risk for knee OA.
Methods: We performed a secondary analysis of Osteoarthritis Initiative (OAI) data. Our exposure was ROA presence (KL grade ≥ 2 vs < 2), at the 48-month visit (analytic baseline, BL). Our outcome was receiving a CS injection assessed using the question “In the past 6 months, have you received a CS injection?” from BL to the 108-month follow-up visit. We excluded participants who answered yes to the CS injection question at BL. PA, measured using an Actigraph GT1M at BL, was examined as an effect measure modifier between ROA presence and CS injection, and 6000 steps/day was used to stratify the sample. We produced Kaplan-Meier survival curves for cumulative incidence of not receiving a CS injection and used Cox proportional hazards regression to calculate discrete-time hazard ratios (HR) adjusted for confounders.
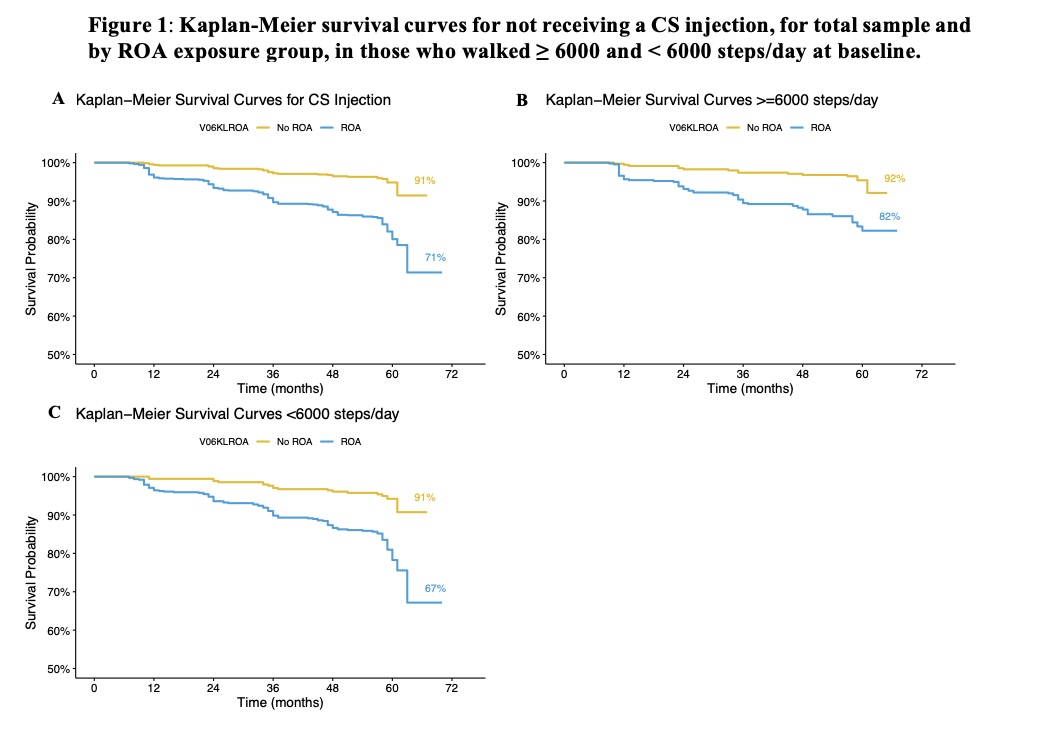
Results: 1763 participants (mean age = 65.0 years old, 55% female, mean BMI =28.5 kg/m2) were included in the overall analytic sample. 204 participants received at least one CS injection over 5 years of follow-up. For participants with ≥ 6000 steps/day, survival probability was 82% for those with ROA and 92% for those without ROA (Figure 1a). Those with ROA had 223% increased hazard of receiving a CS injection compared to those without ROA (adjusted HR [95% CI] = 3.23 [2.05, 5.08]) (Table 1). For participants with < 6000 steps/day, survival probability was 67% for those with ROA and 91% for those without ROA (Figure 1b). Those with ROA had a similar hazard of CS injection whether they walked < 6000 steps/day (3.45 [1.73, 6.89]) or ≥ 6000 steps/day (3.05 [1.66, 5.61]) (Table 2). The interaction term for ROA presence and steps/day was not significant (p = 0.68).
Conclusion: Physical activity does not seem to modify the relationship between ROA presence and CS injection utilization. However, for people with ROA, those who were more active had a slightly attenuated risk of receiving a CS injection than those who were less active as those with ROA who were more active had an 82% chance of not receiving a CS injection compared to a 67% chance for those who were less active over a 5-year period.
.jpg) Note: models were adjusted for age, sex, BMI, race, education, comorbidity, function measured by the Knee Osteoarthritis Outcome Score (KOOS), baseline steps/day, and pain
Note: models were adjusted for age, sex, BMI, race, education, comorbidity, function measured by the Knee Osteoarthritis Outcome Score (KOOS), baseline steps/day, and pain
.jpg) Note: models were adjusted for age, sex, BMI, race, education, comorbidity, function measured by the Knee Osteoarthritis Outcome Score (KOOS), and pain
Note: models were adjusted for age, sex, BMI, race, education, comorbidity, function measured by the Knee Osteoarthritis Outcome Score (KOOS), and pain
To cite this abstract in AMA style:
Liles S, Copson J, White D, Jakiela J. Radiographic Knee Osteoarthritis and Corticosteroid Injection Use: The Moderating Role of Physical Activity [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/radiographic-knee-osteoarthritis-and-corticosteroid-injection-use-the-moderating-role-of-physical-activity/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/radiographic-knee-osteoarthritis-and-corticosteroid-injection-use-the-moderating-role-of-physical-activity/