Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Sinus and nasal symptoms are common and associated with a higher risk of relapse in patients with ANCA-associated vasculitis (AAV). Previously, our group found that a patient questionnaire called the Sino-Nasal Outcome Test-22 (SNOT-22), a validated patient-reported outcome measure in chronic rhinosinusitis, is associated with future relapse even in patients without a prior history of sinonasal disease. A detailed understanding of sinonasal symptoms is still lacking in AAV. The aim of this analysis was to evaluate sinonasal symptom profiles associated with disease activity in patients with AAV.
Methods: Patients with a self-reported diagnosis of AAV were recruited between January and March 2025 through an international research network (Vasculitis Patient-Powered Research Network). Participants rated 26 sinonasal symptoms on a scale from 0 (no problem) to 5 (problem as bad as it can be); the 26 symptoms included the original 22 items from the SNOT-22 plus four additional items related to vasculitis. The 4 vasculitis-specific items were selected based on patient and investigator input and included: nasal crusting, blood-tinged nasal discharge/crusts, nose bleeds, and nasal pain. Total and subdomain scores of the SNOT-22 were compared using linear regression. Sinonasal symptoms associated with active vasculitis versus remission were determined using LASSO-penalized logistic regression. The penalty term (λ) was chosen by 10-fold cross-validation; variables with nonzero coefficients were carried forward into a post-LASSO unpenalized model to estimate odds ratios (ORs) and 95% confidence intervals (CIs).
Results: A total of 663 participants with AAV from 24 countries were included: 130 with active disease, 423 in remission, and 110 who had unknown disease status. Median age at enrollment was 63 years, median disease duration was 8 years, 91% had positive ANCA in the past, and 88% had a prior history of sinonasal disease related to vasculitis. Total and subdomain SNOT-22+ scores were all significantly higher in active vasculitis vs remission group (Figure 1) and remained significant even after adjusting for age, sex, and disease duration. Both groups had higher scores compared to historical healthy control cohorts (mean score 9). Responses to 25 of 26 items were significantly higher in the active vs remission group (Figure 2). LASSO-based variable selection identified 12 items associated with disease activity (Figure 3).
Conclusion: Active AAV is associated with greater sinonasal symptom burden compared to quiescent disease although patients in remission continue to experience higher levels of symptoms compared to healthy patients. More severe nasal pain, more sadness, and less severe sneezing had the strongest association with active disease. A detailed understanding of the sinonasal symptom profile associated with active disease may improve clinical monitoring of disease activity in AAV.
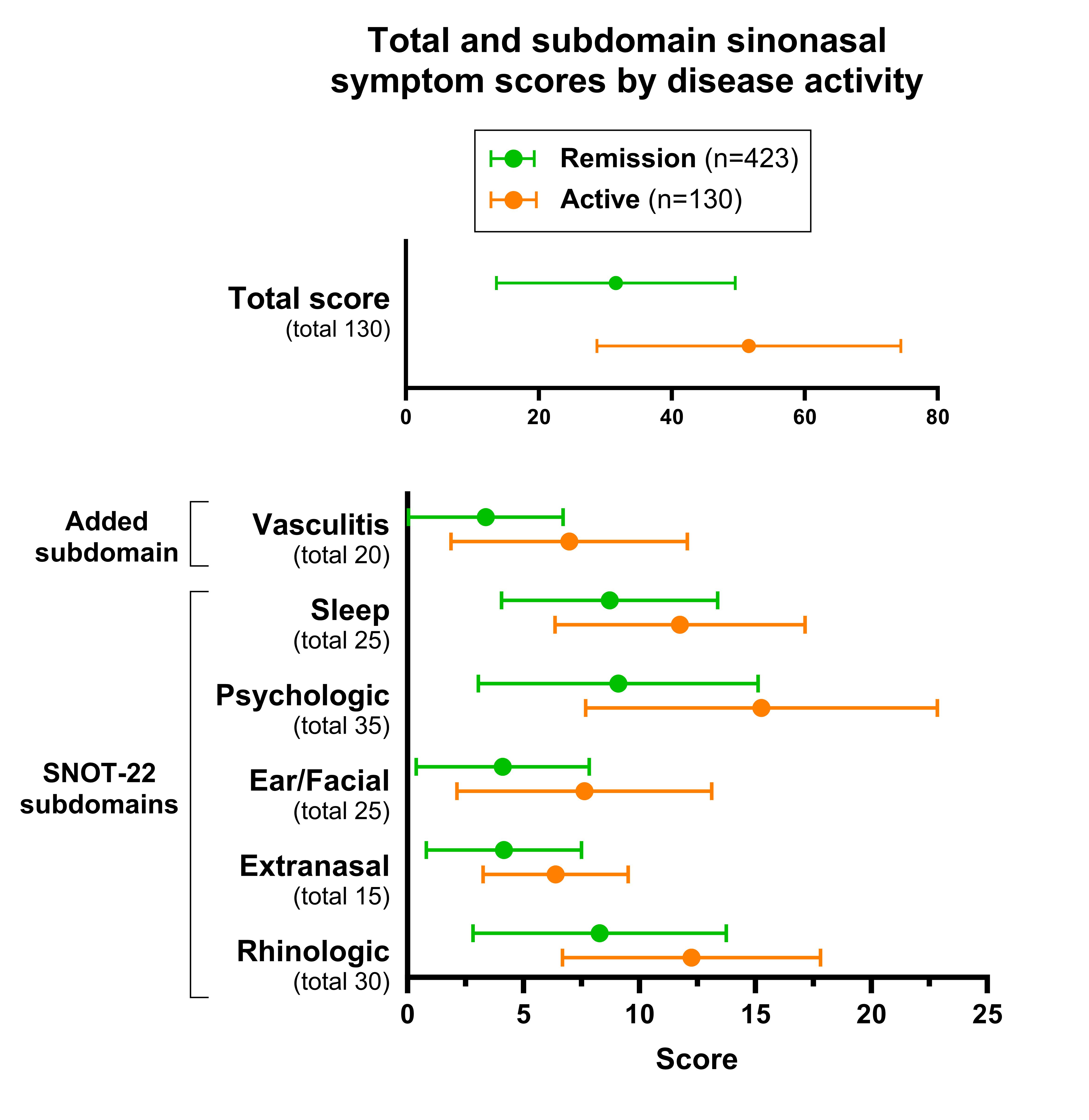 Figure 1. Comparison of Sino-Nasal Outcome Test scores by disease activity in patients with ANCA-associated vasculitis. Mean (SD) of total and subdomain scores from the SNOT-22 plus additional vasculitis-specific questions. Compared to patients with AAV in remission, patients with active disease had a greater burden of sinonasal symptoms and poorer quality of life across all domains (all P < 0.01).
Figure 1. Comparison of Sino-Nasal Outcome Test scores by disease activity in patients with ANCA-associated vasculitis. Mean (SD) of total and subdomain scores from the SNOT-22 plus additional vasculitis-specific questions. Compared to patients with AAV in remission, patients with active disease had a greater burden of sinonasal symptoms and poorer quality of life across all domains (all P < 0.01).
.jpg) Figure 2. Mean response to individual items in the Sino-Nasal Outcome Test by disease activity in ANCA-associated vasculitis. Heatmap depicts the mean response to each item by group (active vs remission). Responses to all items except “wake up tired” were significantly higher in the active vs remission group (all P < 0.05). Items with asterisk and red font were retained in the final model after variable selection.
Figure 2. Mean response to individual items in the Sino-Nasal Outcome Test by disease activity in ANCA-associated vasculitis. Heatmap depicts the mean response to each item by group (active vs remission). Responses to all items except “wake up tired” were significantly higher in the active vs remission group (all P < 0.05). Items with asterisk and red font were retained in the final model after variable selection.
.jpg) Figure 3. Odds ratio with 95% CI for association of sinonasal items with active disease in ANCA-associated vasculitis. Figure displays variables selected in post-LASSO logistic regression model. Nasal pain, feeling sad, sneezing, and lack of good night’s sleep were among the items associated with disease activity in AAV in the multivariable model.
Figure 3. Odds ratio with 95% CI for association of sinonasal items with active disease in ANCA-associated vasculitis. Figure displays variables selected in post-LASSO logistic regression model. Nasal pain, feeling sad, sneezing, and lack of good night’s sleep were among the items associated with disease activity in AAV in the multivariable model.
To cite this abstract in AMA style:
Rhee R, Yeung C, White D, Gibson M, Nguyen J, Burroughs C, Gordon J, Cohen N, Morris J, Merkel P. Sinonasal Symptom Profiles Associated with Disease Activity in an International Cohort of Patients with ANCA-Associated Vasculitis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/sinonasal-symptom-profiles-associated-with-disease-activity-in-an-international-cohort-of-patients-with-anca-associated-vasculitis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/sinonasal-symptom-profiles-associated-with-disease-activity-in-an-international-cohort-of-patients-with-anca-associated-vasculitis/