Session Information
Date: Sunday, October 26, 2025
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Low-dose computed tomography (ldCT) has not previously been used to assess pt with axial spondyloarthritis (axSpA) early in their disease course, especially those with minimal structural damage at baseline. We assessed spinal damage progression using ldCT and evaluate inter-reader reliability in patients (pt) with axSpA.
Methods: In SPondyloArthritis Caught Early (SPACE) cohort, 67 axSpA pt underwent two whole spine ldCT scans over a 2-year follow-up. First scan (T0) took place 0–10 years after inclusion, varying by pt. Regardless of T0 timing, second scan (T2) two years later.Three central readers independently assessed CT syndesmophyte score (CTSS). Readers were blinded to image order and pt data. CTSS calculated per vertebral unit (VU) using eight quadrants, scoring syndesmophytes from 0 (absent) to 3 (bridging the intervertebral disc space), with a maximum CTSS of 552. Inter-reader reliability for CTSS change was calculated using intraclass correlation coefficients (ICC).Changes in CTSS (continuous data) were based on average reader scores and visualized in cumulative probability plots. Dichotomous data (new/growing syndesmophytes) were based on ≥2/3 consensus of readers at vertebral corner level. New syndesmophytes were defined by a score change from 0 to 1, 2, or 3; growth from 1 to 2 or 3, or 2 to 3. Net progression was calculated by subtracting regressors from progressors, divided by total pt, for cut-offs (≥1 to ≥5).
Results: Among 67 pt, 57% were male, 84% was HLA-B27 positive, mean age of 36 (8) years and symptom duration of 6 (3) years. 21% had early axSpA (≤2 years symptoms). For the whole spine, the ICC for the change CTSS was 0.67 (95% CI: 0.50 to 0.78). Segment-specific ICCs showed good reliability for lumbar (0.91, 95% CI: 0.87 to 0.94) and thoracic spine (0.77, 95% CI: 0.65–0.85). Cervical spine showed poor reliability (ICC -1.69 (95% CI: -3.06 to -0.73).Mean CTSS for whole spine increased from 9.6 (18.5) at T0 to 11.2 (20.7) at T2, resulting in a total mean change of 1.6 (4.5). When examining per spinal segments, thoracic spine showed the largest progression with a mean change of 1.0 (3.1), accounting for 63% of total change in the spine. Remaining 38% of spinal damage progression was equally accounted for by cervical and lumbar segments, each showing a mean CTSS change of 0.3 (1.9) and 0.3 (1.5), respectively. Figure 1 shows distribution of CTSS change, with smallest detectable changes of 3.93 (whole spine), 2.42 (cervical spine), 2.33 (thoracic spine) and 0.99 (lumbar spine). Figure 2 shows number of pt with new/growing syndesmophytes per VU. Net progression of new/growing syndesmophytes (consensus) for whole spine was 22% at cut-off ≥1, 18% at cut-off ≥2, 15% at cut-off ≥3, 10% at cut-off ≥4, and 12% at cut-off ≥5.
Conclusion: Whole spine ldCT can detect progression in axSpA, even in pt with short symptom duration and minimal baseline prevalence of damage. Over two years, syndesmophyte progression occurred throughout the entire spine, with net progression rates between 10% and 22%, depending on severity cut-off. The thoracic spine showed the most change, accounting for nearly two-thirds of total progression—more than the cervical and lumbar segments combinedReferences (1) Marques ML, et al. RMD Open. 2024
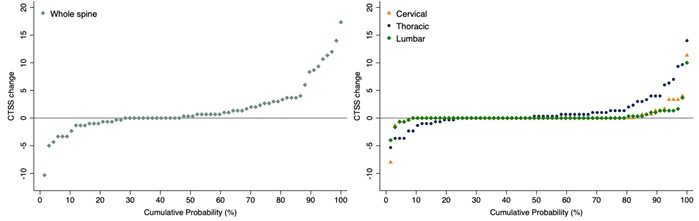 Figure 1. Cumulative probability plots of the change in computed tomography syndesmophyte score (CTSS) over 2 years for the whole spine (left) and separate spinal segments (right), based on aggregated scores derived from the average of individual reader scores
Figure 1. Cumulative probability plots of the change in computed tomography syndesmophyte score (CTSS) over 2 years for the whole spine (left) and separate spinal segments (right), based on aggregated scores derived from the average of individual reader scores
.jpg) Figure 2. Heatmap of spinal progression on ldCT: number of pt with new/growing syndesmophytes (increased red intensity reflects a higher number), based on consensus scores derived from a 2 out of 3 reader majority agreement
Figure 2. Heatmap of spinal progression on ldCT: number of pt with new/growing syndesmophytes (increased red intensity reflects a higher number), based on consensus scores derived from a 2 out of 3 reader majority agreement
To cite this abstract in AMA style:
de Hooge M, Marques M, Ayan G, van Lunteren M, de Bruin L, Reijnierse M, Van Der Heijde D, Ramiro S, van Gaalen F. Low-Dose CT reveals syndesmophyte progression in axial SpA, particularly in the thoracic spine: Insights from the SPACE cohort covering early and established disease [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/low-dose-ct-reveals-syndesmophyte-progression-in-axial-spa-particularly-in-the-thoracic-spine-insights-from-the-space-cohort-covering-early-and-established-disease/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/low-dose-ct-reveals-syndesmophyte-progression-in-axial-spa-particularly-in-the-thoracic-spine-insights-from-the-space-cohort-covering-early-and-established-disease/